





Coronavirus
In early December 2019, a cluster of patients in China’s Hubei Province begin to experience symptoms of an atypical pneumonia-like illness that did not respond to standard treatments.
On December 21st 2019 a 65 year-old deliveryman who worked at the Huanan Seafood Wholesale Market, presented at Wuhan’s central hospital with a pneumonia of unknown origin. On Christmas Eve, samples from his lungs were sent for genetic sequencing and a novel coronavirus was identified.
This marked the start of an unprecedented challenge to global public health systems and caused profound economic, social, and political upheaval. It also led to a rapid evolution in scientific understanding and response around the world.
Where Are We?
The pandemic was declared ‘over’ by the WHO in May 2023. But most people had already abandoned masks, were using crowded public transport, going to events and getting back to ‘normal’ well before that point.
One definition of a pandemic is that it’s an event that changes the way we work, rest and play. Yearly influenza is a perfect example of this: during the 2022–2023 flu season there was a notable surge in hospitalisations and deaths. In a single week that December there were over 2,000 excess deaths in the UK, attributed to flu and related respiratory illness, not to COVID. This barely made the news and nobody changed their behaviour.
We may have ‘forgotten’ the flu and are eager to move past COVID, but we must not overlook the 50,000 to 100,000 immunocompromised individuals in the UK who either cannot receive a vaccine or may not respond effectively to it. Nor should we overlook people with autoimmune or neurological conditions and others at increased risk. While the risk may be significantly lower for most of us, for some infection can still pose serious, even life-threatening consequences.
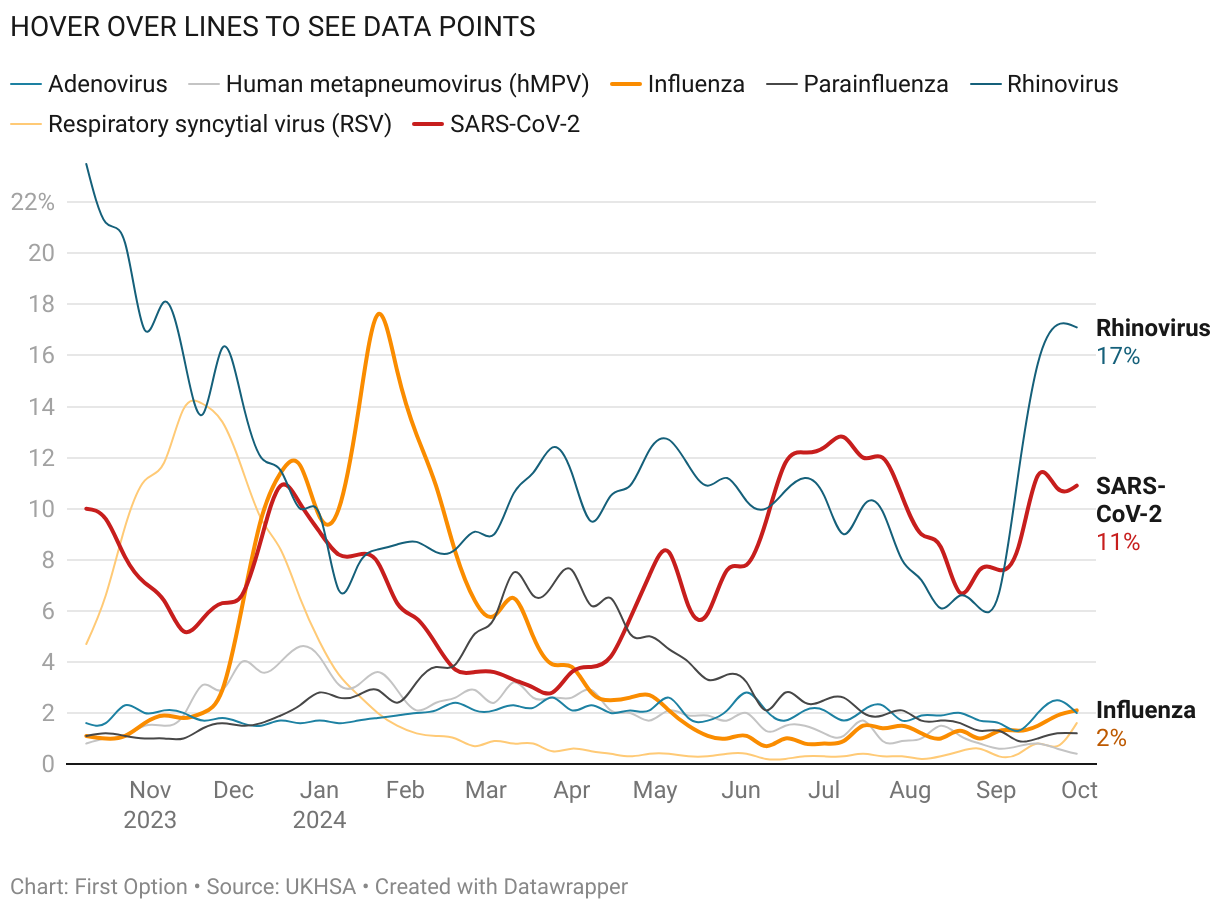
While COVID hasn’t settled into the traditional, seasonal pattern of most respiratory viruses, it’s still likely to spread more in the autumn and winter for the same reasons others do: return to school / college plus various festivals and holidays mean increased mixing across different social groups. Plus we tend to be indoors more and – counterintuitively – respiratory viruses spread more easily in cold, dry air than warm, humid air.
Remember it’s not all about COVID. Other Influenza-Like Illnesses (ILIs) including flu can also disrupt productions.
In Detail
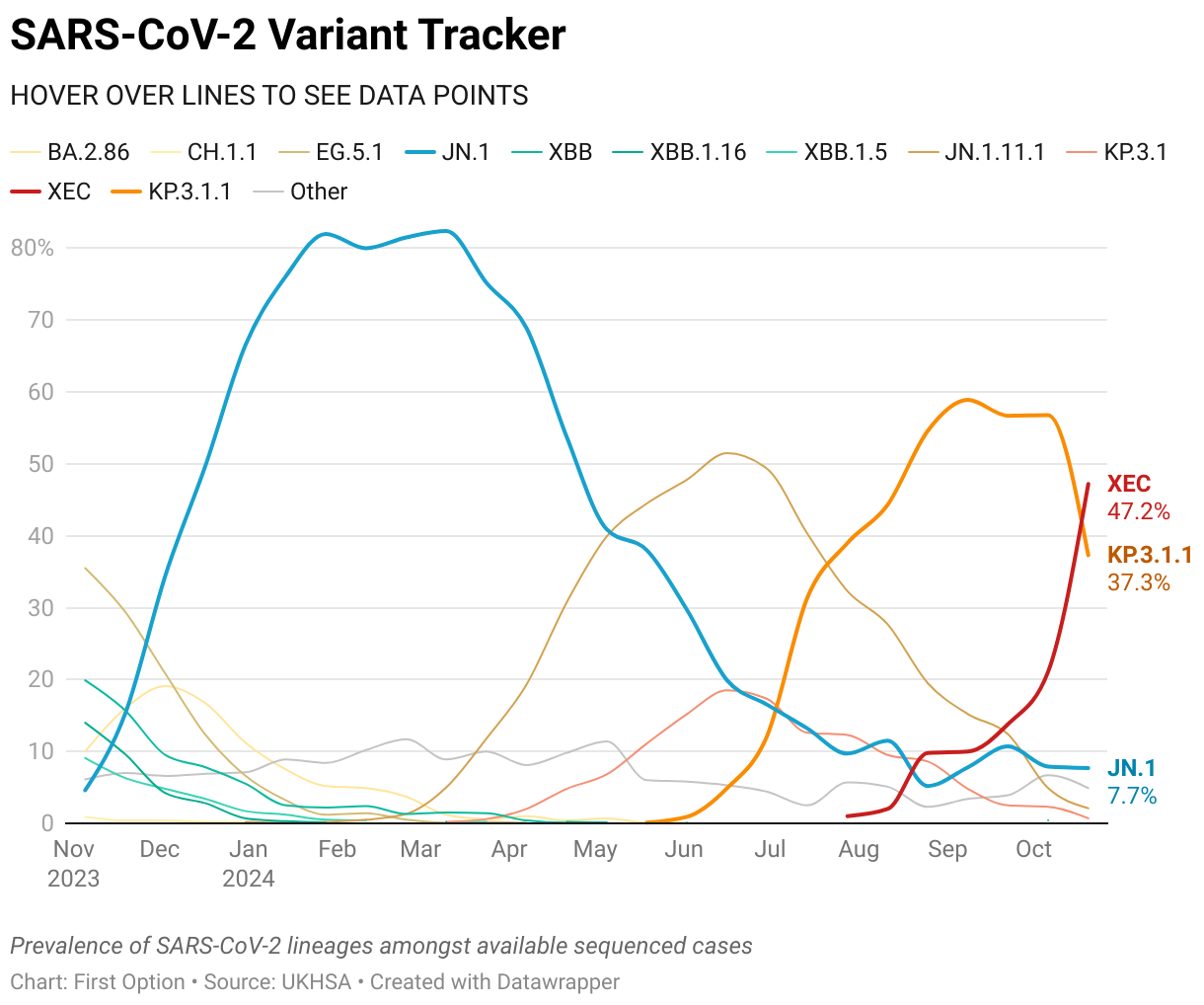
The large-scale, worldwide genetic sequencing of SARS-CoV-2 has been critical to understanding, tracking, and responding to the pandemic. For example sequencing was crucial in identifying the Alpha, Delta, and Omicron variants and understanding their global transmission patterns.
It also helps ensure diagnostics remain accurate and helps development of antiviral drugs and antibody therapies. But the extensive media coverage of every mutation, often accompanied by speculation about its potential impact, led to several issues.
- Media reports often focused on individual mutations, implying that a single mutation could drastically change the virus’s behaviour. In reality, factors like infectivity, immune evasion and virulence result from a combination of multiple factors.
- Mutations that may appear worrisome in a laboratory do not always lead to significant changes in the real world due to other mechanisms compensating for them.
Quite simply, you cannot predict the impact of a particular mutation or suite of mutations until you see how it behaves in a given population. Virus / host interactions are complicated and factors like population density, mobility, and health infrastructure also influence how a variant spreads and causes disease.
The constant media focus on mutations and variants did cause public anxiety. Each new mutation was presented as a potential game-changer, which for many led to a sense of being overwhelmed by the perceived unpredictability and danger of the virus.
Now that some time has passed, we can look back at those predictions and how many were accurate.
D614G Mutation (Early 2020)
- Prediction: early studies suggested that the D614G mutation, one of the first globally dominant mutations, would significantly increase infectivity by stabilising the spike protein and improving viral entry into cells. A tenfold increase in infectivity was predicted.
- Outcome: while the mutation did become widespread, it didn’t lead to a major increase in disease severity or a dramatic boost in transmissibility. But a variant just needs small, incremental gains to flourish and displace others, which is precisely what D614G gave the virus.
N501Y Mutation (Alpha and Beta Variants)
- Prediction: the N501Y mutation, found in both the Alpha (B.1.1.7) and Beta (B.1.351) variants, was predicted to enhance binding affinity to human ACE2 receptors, suggesting higher transmissibility and possibly increased virulence.
- Outcome: although Alpha did exhibit increased transmission, Beta, despite carrying the same mutation, did not lead to the same level of spread or infectivity in many regions. It seems other factors, such as immune evasion or population immunity played a significant role, and the N501Y mutation alone did not dictate these variants’ overall success.
E484K Mutation (Beta, Gamma, and Delta Variants)
- Prediction: the E484K mutation was thought to cause significant immune escape, raising concerns about reduced vaccine effectiveness and higher transmission and/or reinfection rates.
- Outcome: although E484K did show immune evasion in the lab, its impact on transmissibility and severity was not as dramatic as initially feared. For example Delta, which became globally dominant, lacked this mutation, yet was more transmissible than the Beta or Gamma variants carrying E484K.
P681R Mutation (Delta Variant)
- Prediction: the P681R mutation, found in Delta, was predicted to enhance the virus’s ability to enter cells by facilitating spike protein cleavage at the furin cleavage site.
- Outcome: while Delta was highly transmissible, this specific mutation alone could not explain all its characteristics, such as vaccine breakthrough or severity. It was a combination of mutations and factors contributing to Delta’s dominance.
Omicron
When the Omicron variant was first identified in November 2021, several predictions were made based on its unique set of mutations.
Transmissibility
Omicron was predicted to be highly transmissible because it contained numerous mutations in the spike protein, particularly in the receptor-binding domain (RBD). This prediction was confirmed. Omicron became the dominant variant globally within weeks, outcompeting Delta. Its transmissibility was much higher, with a shorter generation time and faster spread in populations. Its multiple sub-lineages (like BA.1, BA.2, and later variants) contributed to successive waves of infection across the globe.
Immune Evasion
The number of mutations in Omicron’s spike protein, particularly in regions targeted by neutralising antibodies from previous infections or vaccinations, it was expected to evade immunity more effectively than earlier variants with a higher potential for reinfection and cases in the vaccinated. This was also borne out. Omicron showed significant immune evasion, leading to a surge in reinfections, including in people who had been infected with earlier variants like Delta or Alpha.
Severity
There were suggestions that Omicron might cause less severe disease based on initial reports from South Africa, where the variant was first detected, and it may finally be that the virus had shifted to a form we could coexist with (like the other, seasonal coronaviruses) rather than cause severe illness.
This wasn’t really borne out by what was observed. Omicron did cause milder disease in some cases compared to Delta, especially in populations with higher levels of immunity (either from vaccines or prior infections). However, it still caused significant hospitalisations and deaths, particularly in the elderly, in those with underlying health conditions, and in areas with lower vaccination rates. Its sheer transmissibility meant that even a small percentage of severe cases resulted in a much larger overall burden on healthcare systems.
Overall…
So, while genomic surveillance and predictive modelling are crucial for understanding potential threats, the true impact of mutations can’t be fully appreciated until we see how they behave in human populations rather than a lab.
On April 1st 2022 the UK Government removed most Coronavirus-specific statutory requirements as part of its COVID 19 Response: Living with COVID. That document set out a roadmap for fully opening up society and ‘living with’ COVID, and there is separate Government guidance for England, Scotland and Wales.
For productions, that means that COVID is now treated just as any other hazard in a workplace. You still need to assess the risk of COVID to your employees and others, and where you assess it as a significant hazard you must ensure appropriate measures are put in place to control it.
It may be that due to the requirements of your production that you look to retain a separate COVID Protocol document. That document should look to list the control measures that you identify in your risk assessment along with other appropriate information. That may include details of any testing regime and the procedures once a positive case has been identified. Its length and amount of detail should be appropriate to your operation.
Where is your risk?
Now that population immunity in the UK is high due to vaccination and/or exposure, and there is no legal requirement to isolate, you should start your assessment by asking “what are the consequences of a positive case on my production / in my workplace?”
Remember that vaccination will not prevent transmission of the virus, or an infection that makes someone sick enough not to be able to work (see below) so you should consider the impact of someone having to take time off sick. For example, if you have talent who may need to take time off due to COVID, how will that impact your production and would you be covered by insurance, as this could pose a potentially significant business continuity risk.
- Who are the key people that are critical to the production staying disruption-free? What can you do to keep them from (a) getting it and (b) coming into contact with anyone who may be infected?
- Identify those who could become ‘superspreaders’ if they become infected. It’s not just cast members or contributors, it’s those working in close proximity too: HMU, costume, unit drivers etc.
Beyond business risk, your highest risk is likely to involve vulnerable persons. These are individuals who, were they to contract the virus, could be at a higher risk to their health due to their individual circumstances. This may include workers who have informed you of their vaccination status.
You will need to assess the work activity based on the personal circumstances of these individuals on a case-by-case basis and decide whether additional measures are appropriate to reduce their risks to an acceptable level.
Control Measures for Consideration
Vaccination
Vaccination dramatically reduces the risk of severe illness, hospitalisation and death. It also significantly decreases the risk of Long COVID. But while vaccination can reduce the risk of transmission and infection, it doesn’t eliminate it.
You can certainly encourage people to have the vaccine (and ACAS has released useful guidance on engaging re this), but because vaccination is not a legal requirement an employer cannot currently require an employee to be vaccinated. Even the Government is barred from forcing individuals to undertake medical treatments such as vaccinations under the Public Health (Control of Disease) Act 1984.
There are circumstances under which employers can ask about vaccination status but these are very limited. Vaccination information is classed as ‘special category data’ under Data Protection legislation and so all employers must comply with this. If you believe you do have grounds to ask this question we urge you to proceed carefully and check with a specialist HR lawyer first.
Ventilation
Make sure that your workplace is well ventilated and do all you can to keep a regular supply of fresh air passing through either through general ventilation or air conditioning. Where you identify poorly ventilated areas in certain indoor locations a specific assessment might be needed. The infection risk may be higher in areas where you cannot easily use general ventilation (utilising open doors and windows) and so you may be reliant on recirculating air conditioning and other mechanical systems.
Face Coverings and Masks
The wearing of face masks and covering is now no longer legally required. However, there may be certain circumstances whereby it is still prudent to consider their use.
Where the risk or consequence of transmission is high and other safety measures are not available, the use of masks should be considered. For example this may include when working in close contact or with vulnerable individuals.
Isolate When Sick
When employees are ill, you should look to encourage them to avoid coming into work. This prevents an infectious person potentially spreading the virus to others in the workplace. In instances whereby it cannot be avoided that a sick person attends (such as required talent) you should assess their workplace to ensure the protection of others. That may include introducing social distancing measures and requiring mask wearing, use of screens and back to back/side to side seating as examples.
Testing
There is a separate section on testing for COVID below.
If a person is ill or showing COVID symptoms they should be encouraged to take a test. If that test is positive, they should look to stay at home and avoid contact with other people. After 5 days (the original test is on day 0), they may choose to take a Lateral Flow Test (LFT) followed by another 24 hours later – if both are negative, and they do not have a temperature, it is likely they are no longer infectious.
Anyone who tests positive should avoid contact with anyone in an at risk group, including if they live in the same household.
Although most people will no longer be infectious to others after 5 days, some people may be capable of passing on an infection for up to 10 days from the start of their illness. They should avoid meeting people at higher risk of becoming seriously unwell from COVID, especially those whose immune system means that they are at higher risk of serious illness from COVID, despite vaccination, for 10 days after the day they took their test and if this is not possible, wear a mask.
Cleaning
Regular general cleaning is still an effective way to protect against COVID as well as any number of other viruses. This should take into account the amount and type of usage that an area has.
It is unlikely that fogging or deep cleans, or regular cleaning of touch points throughout the day will continue to be appropriate or practicable. You may want to look at different options such as providing wipes for wiping down of hot desks and equipment for individuals to utilise before use.
However, daily general cleaning is likely to be sufficient in most circumstances.
Hygiene
Remind people that practising good hygiene continues to play an important part of preventing spread of disease. Look to ensure that the workforce’s access to welfare facilities is appropriate and where necessary look to provide suitable alternatives such as hand gels and wipes.
International Travel
COVID-19 is no longer defined as a global health emergency by the World Health Organization (WHO) and in common with the UK, the vast majority of overseas countries no longer have any in-country COVID-19 restrictions or entry requirements, such as showing proof of vaccination or a negative test.
However, as COVID-19 is still circulating, it’s important to check how the country you’re visiting is currently managing the virus. The FCDO website is a very good start.
You should also check for any COVID-related restrictions on your insurance and make sure you are – as a minimum – covered for any healthcare or repatriation costs.
This should also include the specific legal requirements for entering the country and quarantining as necessary. This may include dedicated isolation rooms in hotels or whether positive cases may need to isolate in a government mandated building. You should also
consider access to healthcare should someone become sick.
You must, as with all work overseas, comply with local law with regard to any isolation or reporting.
Testing on Production
As part of the assessment as to the potential impact of a COVID case on production, you may decide that some form of testing is appropriate to help monitor your team or talent. The exact nature of that testing should be specific to the risk on your production. For example, it might be that you provide testing for talent because they need to work closely without other protective measures. And see our guidance below on testing.
In the case they were to be sick from COVID and require time off, that might trigger a postponement which in turn might not be financially covered. Another might be a contributor with a condition that puts them at higher risk from COVID and who may also be unvaccinated that testing helps to ensure that those working in close contact of the higher risk individuals do not have the virus. The type and frequency of that testing should be decided as part of your assessment.
We’ve written a great deal about testing over the last four years. Different types of test have come and gone but more importantly we have changed, and the virus has changed. We are not the immunologically naïve population we were in 2020 and the virus continually evolves. That which doesn’t kill us mutates and has another go.
Since our immune systems are now primed to recognise and respond quickly to the virus, it’s likely that we’ll show symptoms or become contagious before there’s enough antigen present to trigger a positive result on a lateral flow test.
Many productions have been caught out by this: an individual has symptoms but tests negative and so keeps on working. After 3-4 days they eventually test positive – after they have passed it on to many others on the production.
Why Test?
Why indeed. You have a legal duty to provide a safe workplace, but when a clinician orders a test, they always have two questions in their mind beforehand, and productions may wish to adopt the same mindset when considering testing.
- What is this test actually going to tell me?
- What am I going to do with that information?
We think that PCR has very little utility for productions now. The better lateral flow tests are a good indicator of potential contagion risk in an individual, but because they generally won’t pick up an infection early on, they are better at helping you decide when an individual might be ‘safe’ to return to work. You really can’t rely on LFTs to give an idea whether someone with symptoms poses a risk. If they have symptoms, assume they probably pose a risk of transmission.
Here are your options – which we’ve considerably simplified and truncated.
Reverse Transcriptase Polymerase Chain Reaction (RT-PCR)
This test looks for genetic material (RNA) from SARS-CoV-2 in a sample, and if it finds any it will repeatedly duplicate it until there is enough present for the detector in the machine to ‘see’ it. The ‘RT’ part is because SARS-CoV-2 has RNA as its genetic material, this needs to be ‘reverse transcribed’ into DNA for PCR to amplify.
- Despite claims that PCR is the ‘most accurate‘ or ‘gold standard‘ test, it really isn’t in terms of how meaningful it is for a production. It is if someone presents at A&E with a high fever and a clinician needs to know if it’s flu or COVID, but in terms of question (1) above, on a production it can tell you if someone has been exposed to the virus recently (and in some cases, months ago) but PCR really does not speak to how infectious a person might be, or what risk they might pose.
- Early on, statements by the NHS that “if you test positive, you have COVID-19” were inaccurate at the time (and remain so now) but helped fuel widespread misconceptions.
If clients think PCR has utility in a production, please contact us and we’ll talk it through with you.
Antigen Tests (LFTs / LFDs)
These measure viral protein – antigens – usually the nucleocapsid protein because it’s the most abundant.
- You need quite a lot of antigen to be present to identify a positive.
- A line is a line. If the test line appears alongside the control, the individual has tested positive. You cannot tell from the appearance of the line how contagious someone is. Faint line? Still positive.
- A positive test result correlates well with infectiousness – but a negative one in a symptomatic individual does not mean they are not potentially contagious.
- These are unlikely to reliably pick up an infection early on – usually they will identify a positive some days after symptom onset – and so are better used as a ‘safe to return’ rather than a ‘safe to work’ test.
In terms of how predictive they are, here are some statistics regarding performance in an adult population with good immunity. This will vary by test and by individual, but it gives an idea. The two percentages give an indication of accuracy for lower / higher viral loads.
| Symptom Onset | Day 0 | Day 1 | Day 2 | Day 3 | Day 4 |
|---|---|---|---|---|---|
| LFT Sensitivity % | 30.0/60.0% | 53.5/80.2% | 59.2/74.8% | 80.0/93.3% | 80.6/90.3% |
Legals
The law surrounding testing has changed multiple times over the course of the pandemic. The Government of the time said this was to ensure quality and safety, but it also had the effect of consolidating both manufacture of tests and provision of testing in the hands of fewer, larger providers.
Productions should be aware that even private GPs, set medics and other qualified medical professionals are barred from conducting simple COVID tests as part of their clinical practice outside the NHS unless they clear significant barriers to entry.
Here’s what you need to know (but is not legal advice):
Under The Health Protection (Coronavirus, Testing Requirements and Standards) (England) (Amendment and Transitional Provision) Regulations 2023, if you’re subcontracting sample taking and/or sample analysis, the subcontractor needs to possess the relevant ISO standard and be registered with UKAS, or another accreditation body recognised by the International Laboratory Accreditation Cooperation (ILAC). These are:
- “in relation to sample collection or a point of care test, ISO Standard 15189:2022”
- “in relation to a diagnostic laboratory, either ISO Standard 15189:2022 or ISO/IEC Standard 17025:2017”
There are carve outs:
- This does not apply to self-administered, ‘home’ COVID tests that can be purchased in chemists etc. It only applies if you’re subcontracting sample taking and/or sample analysis to a third party such as a set medic.
- It also does not apply if you testing programme is entirely in house – that is, you’re not subcontracting sample taking and/or sample analysis to a third party.
We urge productions to take care navigating this minefield and to take professional advice if outsourcing any testing.
By mid-January 2020, the bat coronavirus that entered the human population in China in late 2019 had been identified and its genome sequenced. This ‘Wuhan-1’ or ancestral strain is the one on which all vaccines were based. But that’s not the virus that infected the world.
Early in the pandemic a mutation cropped up called D614G (it’s so called because at position 614 in the virus spike protein a mutation caused a switch from aspartate ‘D’ to glycine ‘G’).
This single change helped SARS-CoV-2 to rapidly establish itself globally. It made the virus more stable and gave it an increase in contagiousness. D614G was replaced by Alpha, then Delta, then we swept through most of the Greek alphabet with each iteration being more contagious than the last.
We covered in the previous section why, in diseases with short incubation times, vaccines cannot completely protect against mild disease and transmission, but are very good at preventing severe illness and death, and COVID vaccines continue to do just that irrespective of variant due ti T and B cell-mediated immunity.
How were the vaccines developed so quickly? Were corners cut? Was safety compromised?
Governments hedged their bets with vaccines to counter a novel and serious threat. The ‘new’ mRNA vaccine technology (which in fact had been in development since the 1970s) had the potential to be the fastest to market: as soon as you have the genetic sequence of the virus you have the potential to make a vaccine. Indeed this approach was being used in HIV vaccine research since the early 2000s.
But Governments also ordered more traditional protein subunit vaccines as well as adenovirus vector vaccines (where you reprogramme another virus to deliver antiviral software directly into human cells, which then deletes itself like a Snapchat message once the code has been executed). Adenovirus vector vaccines were already in trials for HIV, Ebola, influenza virus, TB and malaria. The AstraZeneca and Johnson & Johnson vaccines use this platform.
If RNA vaccines had been in development for decades, why now?
In 2023 Katalin Karikó and Drew Weissman were awarded the Nobel Prize in Physiology or Medicine for their discoveries concerning nucleoside base modifications that enabled the development of effective mRNA vaccines against COVID-19.
The SARS-CoV-2 spike protein is inherently unstable. Weissman et al added two ‘stiff’ amino acids to stabilise it.
The second issue is that RNA sets off a massive inflammatory response. RNA has four building locks: adenine, guanine, cytosine and uracil. Karikó solved this major obstacle by substituting the uracil with pseudouridine. Without these two individual breakthroughs, mRNA vaccines would not have been possible.
In addition to spread betting across manufacturers and vaccine technologies, Governments also underwrote all development and trial costs. This meant trial mRNA vaccines were being tested on monkeys and mice within weeks of the SARS-CoV-2 RNA sequence being released.
The problem is (as any biologist will tell you) monkeys exaggerate, and mice lie. So then you need Phase 1 ‘dose ranging’ studies in about 100 people to test safety, make sure the participants don’t grow another head, look for any obvious side effects, and establish best dosage and timing of the new treatment.
To make sure the vaccine consistently elicits a response you then give it to a few hundred people. This is Phase 2 and asks “does drug or vaccine X improve / prevent disease Y?”
To get any pharmaceutical to Phase 3 – which involves recruiting tens of thousands of people to test – has already cost a huge amount of money. The BMJ recently quoted a median figure of $48m for a Phase 3 trial, but it can easily be twice that. Pharmaceutical companies tend to be cautious and plan trials meticulously, because having to repeat them if the regulator has any objections to their methodology is wildly expensive. This is the principal reason drug and vaccine development takes so long.
A typical vaccine development timeline is 5 to 10 years – and sometimes longer – to assess whether the vaccine is safe and efficacious in clinical trials, complete the regulatory approval processes, and manufacture sufficient quantity of vaccine doses for widespread distribution.
But for COVID vaccines, Phase 1 and Phase 2 were combined, and then manufacturers went directly to Phase 3 trials and started manufacture, on the assumption their vaccines would work. It isn’t usually done that way.
If a candidate vaccine failed in Phase 3, then millions of doses would have been thrown away – but at no cost to the manufacturer. So the reason we had vaccines so quickly isn’t because they weren’t trialled properly or that corners were cut or that safety was ignored, it was because Governments, manufacturers and regulatory bodies worked together to turn it around in record time.
Were the vaccines tested properly?
Full clinical trials for mRNA COVID-19 vaccines were carried out before they were approved by regulators and rolled-out to the public. Pfizer’s trial enrolled over 45,000 participants across the globe and Oxford recruited over 23,000 people in the UK, Brazil, and South Africa.
Regulators insist that participants in Phase 3 trials are monitored for a minimum of two months after their final dose to ensure there are no unexpected side effects that take time to manifest themselves. Was that the case with COVID mRNA vaccines?
In the USA, the then President Trump tried to overturn this rule so the vaccines would be available before, not after, the presidential election that November. But the FDA stood firm. The rules were followed.
The irony that given Trump’s antivaccine rhetoric before that point (and since) he would try to co-opt vaccines for political gain was not lost at the time on the scientific, medical and safety communities.
What about boosters?
Boosters for COVID-19 have been recommended primarily to address waning immunity or to provide additional protection against new variants, but these boosters are not required on an annual basis like a flu shot, as immune protection against severe COVID illness generally remains effective for longer.
Different countries also have different strategies: in the UK, boosters are offered to the most at-risk groups (the elderly, the immunocompromised) and healthcare workers. The USA has traditionally relied far more on preventative medicine – including vaccination – because access to access to treatment can vary significantly based on factors such as employment, income, and geographic location. Many individuals, especially those without health insurance or those living in rural areas may have limited access to healthcare services.
As long as T and B cell responses remain strong we are less in need of boosters. This is unlike flu where high mutation rates and the unpredictability of circulating strains each season mean that public health strategies aim to reduce the overall burden of flu by vaccinating annually.
Side Effects
Vaccines can cause side effects. Usually these are mild and self-resolving – a sore arm, malaise etc. But sometimes there can be serious side effects: oral polio vaccine causes rare cases of polio but is easier to distribute than the injected version, which can make a big difference in disaster zones or remote areas. There was a flu jab some years ago that caused rare cases of narcolepsy. Serious side effects are very rare because any adverse signals tend to get picked up in Phase 3 trials because tens of thousands of doses are given.
This is also why trial participants are monitored for a minimum of two months after their last dose. If something is going to happen, it will within that time. But if your Phase 3 trial involves tens of thousands of participants, it may not pick up a one-in-a-million side effect. You may not see that until it’s been in a few million arms.
Myocarditis
One of the few adverse events associated with the mRNA COVID vaccines manufactured by Pfizer-BioNTech and Moderna was an increased risk of myocarditis (inflammation of heart muscle) or pericarditis (inflammation of the lining around the heart).
To quantify this, an analysis of 11 separate studies involving over 58.6 million people. Among its findings were:
- The risk of developing either myocarditis or pericarditis increased following COVID-19 vaccination.
- Risk was greater in men than women, and in people under 40 years vs over 40.
- Risk was statistically significant for myocarditis, but not pericarditis.
- Risk was only significant in the mRNA vaccines, in others.
But to understand the numbers, we need to understand two things.
- Is the risk greater than the background rate? People have heart attacks, strokes etc so much that we know the expected rate of such things. Is that rate higher in the vaccinated vs the unvaccinated.
- Getting COVID also increases the risk of myocarditis and pericarditis. Which carries more risk? The vaccine or COVID itself?
The risk of myocarditis following one of the mRNA vaccines is about 40 cases per million doses (0.004%) among younger men (the highest risk group), – which is a very low number. The rate was 2.4 and 1 per million doses in older men and women, respectively.
If we look at the statistics for mRNA vaccines in young males, 11,000 COVID cases, 560 hospitalizations, 138 ICU admissions, and six deaths due to COVID-19 could be prevented, compared with 40 cases of myocarditis, where over 90% would make a complete recovery. The vaccination also hugely reduces the risk of Long COVID and other comorbidities.
But COVID also causes myocarditis. There are 1,500 cases per million COVID infections vs 40 per million in the high-risk group (young males). So the benefits of the vaccine would seem to hugely outweigh the small risk of self-limiting illness.
Blood Clots I
Cases of venous thromboembolism (VTE) following mRNA-based vaccination were reported in 2022 after COVID-19 vaccines were administered in the US and some other countries1 2 3 4. However, VTE is a common condition that affects 1 to 2 per 1,000 people each year. That means that in a period of widespread vaccination, some cases of VTE will occur shortly after vaccination by chance alone.
A very large study looked at the associated between VTE and vaccines and found no association between mRNA COVID vaccination and venous thromboembolism.
Blood Clots II
The adenovirus vector vaccines (J&J / Janssen and Oxford-AstraZeneca) were associated with a type of blood clot called cerebral venous sinus thrombosis (CVST), in combination with low levels of blood platelets (thrombocytopaenia). This was a very rare autoimmune reaction in women less than 50. The European Medicines Agency quoted 222 cases in 34,000,000 people vaccinated so about 1 in 150,000. This was identified quickly and those at risk were switched to other vaccines.
Association Fallacy
Despite no association between mRNA vaccines and VTE, and a limited association between adenovirus vaccines and thrombocytopaenia in a small group that was quickly identified and solutions put in place, the misconception that vaccination causes blood clots has become commonplace. Additionally, reports that broadly link vaccines with thrombotic events may cause people to falsely associate blood clots as a side effect with all available vaccines. This may be another cause of vaccine hesitancy.
It should also be stressed that any infection can trigger thrombotic events. After respiratory and other infections, people have a 3–6-fold increased risk of arterial thrombosis, such as myocardial infarction and ischaemic stroke, and a 2–3-fold increased risk of venous thromboses, such as deep vein thrombosis of the legs and pulmonary embolism. But due to its mode of action, a heightened risk for thrombosis seems to be a particular hallmark of COVID.
A SARS-CoV-2 infection has a number of distinct phases.
Incubation Period
The Incubation Period is the time between exposure to the virus and symptom onset. It can be anything from 2-14 days. While newer variants and greater levels of specific immunity (due to prior exposure and/or vaccination) may be associated with more people developing symptoms in the first few days after exposure, there are still individuals not testing positive until near the end of this 14 day period. If a person reaches day 14 and is not testing positive, the likelihood of having acquired an infection has most likely passed.
A well described aspect of SARS-CoV-2 is its ability to generate subclinical (or asymptomatic) infection with transmission despite no obvious symptoms.
Asymptomatic transmission prior to or without ever progressing through the early clinical phases was documented early on in the Diamond Princess Cruise Ship Cohort and in other contact tracing and modelling studies.
Early Viral Upper Respiratory Non-Hypoxic Phase
The Early Viral Upper Respiratory Non-Hypoxic Phase is the first clinical stage when individuals test positive and/or develop upper respiratory and other viral symptoms. This is the mild or moderate stage of COVID-19, but certain individuals can progress to severe or critical COVID-19 – especially the unvaccinated.
During this phase it presents as an influenza-like viral illness with a mix of fever, headache, sore throat, nasal congestion, cough, myalgia, fatigue, loss of taste and smell and gastrointestinal symptoms. Multiple well-designed studies have demonstrated that this is the critical period to initiate antiviral therapies, such as Paxlovid or monoclonal antibodies (but as the virus spike mutates, individual monoclonals can become less effective or ineffective but Paxlovid is holding strong).
The timing of symptom onset and test positivity may be influenced by the specific viral variant, prior infection status, vaccination status or the individual that has been infected.
People who have mild COVID-19 tend to see an improvement in their fever and cough after a week or so, but in more serious cases the disease can progress further.
Early Inflammatory Lower Respiratory Hypoxic Phase
The Early Inflammatory Lower Respiratory Hypoxic Phase is far less common now that at the beginning of the pandemic. This is the phase that put people in the ICU – or the mortuary. It generally begins during the second week, but has earlier onset in the elderly and those with comorbidities, and later onset in younger, healthier individuals.
By this stage, viral replication has all but ceased – it’s the body’s (over)reaction to the infection that makes us so ill. It’s the immune system going into overdrive.
The first obvious clinical manifestations of this phase are usually pulmonary, with the onset of hypoxaemia, then increasing respiratory rate and then increasing hypoxaemia, which in many cases can be rapid and require significant supportive care, and pulmonary support is the primary reason for hospitalisation.
In untreated individuals this can progress to cardiac dysfunction, kidney failure, neurological manifestations, and multi-organ dysfunction or failure. There is usually a rise in inflammatory markers that can be picked up with blood tests and this often described as the ‘cytokine storm’.
It is during this period that corticosteroids have been shown to reduce the risk of progression to critical disease and death. However, early in the pandemic the premature use of steroids during the first week of illness was later associated with significant harm.
Secondary Symptomatic Phase
The Secondary Symptomatic Phase is a period during when there may be significant inflammation. Complications during this period are the Multisystem Inflammatory Syndrome in Children (MIS-C) and the Multisystem Inflammatory Syndrome in Adults (MIS-A), vasculitis, Guillain-Barré syndrome, facial palsies and immune-mediated thrombocytopaenia.
Late Phase
The Late Phase may be a continuation of the acute period for some, or improvement followed by worsening or recurrence of symptoms for others, or for some it might be a novel presentation after a minimally symptomatic or asymptomatic acute experience. In general, the Late Phase is the period of time most associated with the development of Long COVID (or ‘post-acute sequelae SARS-CoV-2 infection (PASC)).
‘Paxlovid Rebound’
‘Paxlovid Rebound’ was described as a resurgence of COVID-19 after you finish taking the antiviral drug combination known as Paxlovid – either COVID-19 symptoms returning or testing positive after testing negative. Or sometimes both.
This early attribution of a post viral syndrome to Paxlovid has been crushed by subsequent data. It turns out ‘Paxlovid Rebound’ doesn’t exist: multiple studies have shown that this sort of rebound is equally common in people who haven’t taken Paxlovid as it is in those who have. Many viral infections are associated with a post-viral syndrome. COVID is no different.
But COVID rebound is a clinical syndrome that does exist. It is defined as a recurrence of symptoms and/or receiving a positive COVID test after having the disease and then testing negative. It has been reported to occur between two and eight days after initial recovery, including in people who were up to date on their COVID vaccinations.
It’s characterized by a brief surge in symptoms that might last a few days, so it’s different from Long COVID which involves new, returning, or ongoing symptoms that can include a wide range of ongoing health problems and may last days, months, or even years.
Also multiple studies have shown that Paxlovid – when prescribed at the right time – reduces hospitalisation and death by 86% in unvaccinated COVID patients, and by 80% in those who have been vaccinated. In November ’22, the CDC reported that adults who took Paxlovid within five days of a COVID diagnosis had a 51% lower hospitalization rate within 30 days, compared to those who did not receive the drug.
The challenge is that this unfounded fear may cause people to avoid Paxlovid through fear of rebound, but for high-risk patients the benefits of Paxlovid in preventing severe disease, hospitalisation and death far outweigh the downsides of a COVID rebound, which is usually mild, has nothing to do with Paxlovid, and will usually do nothing more than prolong your isolation period.
Long COVID
While the acute manifestations of infectious diseases are well known, in some individuals, symptoms can either persist or appear after the acute period. Post viral fatigue syndromes are recognized with other viral infections and can occur after COVID-19 too.
There are a growing number of individuals with symptoms that persist for weeks, months, and years. Post-acute sequelae of COVID-19 (PASC) is defined by the WHO as the ‘continuation or development of new symptoms 3 months after SARS-CoV-2 infection, with symptoms lasting for at least 2 months with no other explanation’.
There is a correlation between Long COVID brain fog, muscle pain, and longer time to clear SARS-CoV-2 RNA from the upper respiratory tract during acute infection. There is also evidence of disturbance in the gut microbiome, leading to the suggestion that this is a significant factor driving the development of long COVID.
There is further evidence of ongoing neural dysfunction – particularly involving the vagus nerve – in individuals with long COVID. This may explain symptoms such as cognitive dysfunction, oesophageal reflux, tachycardia, orthostatic hypotension, dizziness, dysphonia, dysphagia, and dyspnoea. Ultrasounds in some individuals show thickened and hyperechogenic vagal nerves along with reduced intestinal peristalsis.
Long COVID certainly exists and a fuller picture of it is emerging. But the good news is that COVID-19 vaccines consistently prevent long COVID symptoms in adults by over 50%.
Ever since the first reports of what was later named SARS-CoV-2, there has been intense speculation surrounding its emergence in the human population. Debate has coalesced around two competing ideas: some sort of laboratory escape (whether accidental or deliberate), and spillover from an animal reservoir (zoonotic emergence).
As time goes on, more and more peer-reviewed papers in high-impact journals have emerged supporting zoonotic spillover 1 2 3 4 5 6.
It has now even been established the corner of the market that was the epicentre of that spillover7 8 : it was where wild mammals were being sold. So the evidence points to SARS-CoV-2 emerging in precisely the sort of environment one would expect it to – and in a manner scientists have been warning about for years.
No evidence has emerged supporting a lab leak. In fact all the data points towards that not being the case. But the coincidence that a virology lab was a mere 10km away many find just too compelling.
For those that are interested, here’s a summary of the the arguments and data, which we’ve tried to summarise and explain.
In early December 2019, a bat coronavirus arrived in Huanan, South China. It was quickly established that this was a novel coronavirus, and medics were becoming increasingly concerned. It killed over 4,000 people before it left China – and the rest is history.
On January 1st 2020 the Huanan market was closed by the authorities for ‘sanitation and renovation’.
On that same day the health commission of Hubei province instructed genetic sequencing labs to “stop testing and destroy all samples”. This hampered research into the origins of SARS-CoV-2 enormously. But we do need to remember that at this point the anti-Chinese rhetoric from some Western leaders hardly fostered a spirit of cooperation and was the start of the politicisation of the pandemic.
Some have questioned whether the authorities’ actions were to contain a dangerous virus, or dangerous information – but if it’s the latter, it is more likely that the dangerous information concerns the sale of wild animals rather than the Wuhan Institute of Virology.
The live wild animals trade is illegal in China, but the market is worth billions and officials have traditionally turned a blind eye. It is noteworthy that the Chinese Government insisted that references to live animal sales were kept out of the WHO summary report, despite voluminous evidence of it having been happening at the Huanan market for years.
The Case for Lab Escape
It’s true that there have been isolated cases of infectious agents escaping from labs. Many have seized on the fact that the Wuhan Institute of Virology (WIV), 10km south of the Huanan market and on the other side of the Yangtse river, conducted research into coronaviruses. Surely that cannot be a coincidence?
In terms of evidence, the challenge is that there is no epidemiological link to the WIV and none of the workers there had developed antibodies to SARS-CoV-2 when they were tested. The closest viral sequence to SARS-CoV-2 at the WIV was called RaTG13, sampled from a Rhinolophus affinis bat in Yunnan in 2013.
Many have claimed RaTG13 is the origin of SARS-CoV-2, but that doesn’t stand up to scrutiny.
- RaTG13 is a partial genetic sequence, not a whole virus, so it cannot have been cultured or grown. It’s a fragment of RNA isolated from bat poop in a cave. You can’t grow a whole virus from a fragment of a genome.
- The RaTG13 sequence collected by the WIV has a genetic distance of ∼4% (∼1,150 mutations) from the original Wuhan-Hu-1 SARS-CoV-2, reflecting at least 40 years of evolutionary divergence.
- Three other bat viruses—RmYN02, RpYN06, and PrC31—are far closer genetically and thus share a more recent common ancestor with SARS-CoV-2 than does RaTG13. None of these were at WIV and all were sequenced after the pandemic began.
So, RaTG13 cannot have been the progenitor of SARS-CoV-2, with or without lab manipulation. And no genetic sequences similar to SARS-CoV-2 were at WIV. And the lab was genetically evaluating (sequencing) viral genomes from animal samples: this isn’t the same as growing or working with live virus.
The Case for Genetic Engineering
One conspiracy theory is that a highly unpleasant new strain of COVID was engineered at the WIV and deliberately released on the world by – well – who knows. Some versions of this cast Anthony Fauci, one of the most respected infectious disease experts in the world, as the ‘Dr Evil’ figure at the centre of this. The problem with this hypothesis is those promoting it don’t have even the most basic understanding of molecular biology.
A principal reason SARS-CoV-2 is so infectious is because it has something called a furin cleavage site (FCS) in its spike. A number of viruses use this trick to aid entry to mammalian cells, and it makes them all very transmissible. Some say that this FCS was artificially engineered into SARS-CoV-2. This idea is problematic for a number of reasons.
- In order to do this in a lab you’d need to grow the virus in cell culture. This is a rather finicky task and one of the very few vehicles you can use for this are called Vero E6: kidney cells from African green monkeys. But growing SARS-CoV-2 in Vero E6 consistently results in the loss of the furin cleavage site. Which is rather inconvenient for this particular conspiracy theory.
- So let’s say that to get around this insurmountable problem ‘they’ performed an unusual and unnecessarily complex feat of genetic engineering to add the FCS back in.
The SARS-CoV-2 FCS is what’s known in the trade as an ‘out of frame’ insertion which results in the loss of a single amino acid (an arginine) in its structure. This loss means the original Wuhan virus FCS was far less efficient than those of other human coronaviruses already in circulation. So if this was manufactured ‘they’ engineered in a really very poor FCS in such a way that even your worst postdoc wouldn’t. It just doesn’t stack up.
- Yes, viruses are subject to genetic engineering tricks in labs for many benign reasons. This is how we find out how they work and how to deal with them. But such techniques leave very distinct genetic fingerprints which really aren’t difficult to detect – and SARS-CoV-2 has none of these tell-tale traits.
And no, you can’t just engineer a whole virus from scratch. Such technology is the stuff of science fiction. It’s just not a thing.
Were that not enough to scupper the ‘engineered / enhanced’ school of thought, if we look at the other fitness enhancements we’re seen in each new variant, they all evolved during the pandemic. This is a signature of ongoing adaptation of a virus circulating in humans. The original Wuhan strain was just about good enough to spread in a dense population of immunologically naïve hosts. All the serious adaptation came later through evolution.
Also, no epidemic has ever been caused by the escape of a novel virus, and there is no data to suggest that the WIV or any other laboratory was working on SARS-CoV-2 – or any virus similar enough to be its progenitor – prior to the COVID-19 pandemic.
Quite simply, the idea of a lab leak – of an engineered virus or not – is incompatible with observed clinical, genomic, and epidemiological data. There is neither evidence that any early cases had any connection to the WIV, but they did have clear links to animal markets in Wuhan. Nor is there evidence that the WIV possessed or worked on a progenitor of SARS-CoV-2 prior to the pandemic.
The Case for Zoonotic Origin
Coronaviruses have long been known to present a high pandemic risk. SARS-CoV-2 is the ninth coronavirus known to infect humans and the seventh identified in the last 20 years 9 10. All previous human coronaviruses have zoonotic origins (as do the overwhelming majority of human viruses).
SARS-CoV-2 displays clear similarities to a SARS-like coronavirus that spilled over into humans in Foshan, Guangdong Province, in November 2002, and again in Guangzhou, Guangdong province in 2003. Both these SARS-CoV emergence events were associated with markets selling live animals, particularly civets and raccoon dogs which are well known to be susceptible to SARS-CoV-2 infection. During 2019 markets in Wuhan—including the Huanan Seafood Wholesale Market—traded many thousands of live wild animals including high-risk species such as civets and raccoon dogs.
Following its closure, SARS-CoV-2 was detected in environmental samples at the Huanan market, primarily in the western section that traded in wildlife and domestic animal products, as well as in associated drainage areas including hog badgers, red foxes – and raccoon dogs were consistently available for sale in November and December 2019.
In fact, it wasn’t one virus. There were two lineages – A and B – that circulated contemporaneously and were the result of at least two separate cross-species transmission events into humans. This is also rather unhelpful to the lab leak protagonists’ arguments.
Lineage B became dominant globally and was observed in early cases linked to the Huanan market and the environmental samples taken there. Lineage A was associated with other markets and with later cases in Wuhan and other parts of China. This pattern is consistent with the emergence of SARS-CoV-2 involving multiple spill-over events with infected animals and/or traders, as potentially infected animals were moved into or between Wuhan markets via shared supply chains and subsequently sold for human consumption.
It also mirrors the emergence pattern of the 2003 SARS-CoV. The only missing link is that no bat reservoir or intermediate animal host for SARS-CoV-2 has been identified so far (and can’t be due to the market being shut before animals could be sampled). But subsequent analysis has identified the SARS-CoV-2 genome alongside the mammals that were present too
The absence of a feral intermediary between bats and us is not suspicious in and of itself. It’s just that the right animal species and/or populations haven’t been sampled yet, and/or the virus may be at low prevalence. In fact, the virus may have burned through the intermediate host and we’ll never know. This is very common in the study of zoonotic viruses.
The animal origins of many well-known human pathogens including Ebola virus, hepatitis C virus, poliovirus, and the coronaviruses HCoV-HKU1 and HCoV-NL63 are yet to be identified. It took over a decade to discover bat viruses with >95% similarity to SARS-CoV that were able to use the human ACE-2 receptor as the means to gain entry to host cells.
We may never identify the actual reservoir (despite knowing many bat species are full of coronaviruses) or an intermediate host. This virus is a remarkable generalist due to the ACE-2 receptor it binds to being present in so many mammals. It will burn through a susceptible population of a particular species and then disappear and then reappear somewhere else – just like the Ebolaviruses do.
These spillover events occur constantly and almost all go undetected and do not lead to sustained onward transmission. In fact, only a very small fraction of spillovers from animals to humans result in major outbreaks.
This one just got lucky.
Conclusion
Just as is the case for the vast majority of viruses that infect humans, the most parsimonious explanation for the origin of SARS-CoV-2 is a zoonotic spillover event. All the evidence points unavoidably to that.
The suspicion that SARS-CoV-2 might have a laboratory origin seem to stem entirely from the coincidence that it was first detected in a city that has a major virological laboratory that studies – amongst other things – coronaviruses. And that’s it. It’s a suspicion with absolutely no evidence to back it up.
The influenza virus and SARS-CoV-2 have some superficial similarities. Both spread in a similar way. Both have RNA as their genetic material. Both present initially with similar symptoms. But despite these similarities they are very different in terms of their effects at both individual and population level.
First, don’t underestimate flu. Flu – the illness caused by infection with the influenza virus, not ‘man flu’ – kills. It preferentially kills the old, the young, the infirm, the obese and the pregnant, but it kills the healthy too by making other conditions worse and killing indirectly via acute secondary infections, increasing risk of vascular events like stroke and heart attack and by worsening underlying diseases like congestive heart failure and chronic bronchitis.
The 2009 (A)H1N1 Swine Flu killed in excess of 250,000 – but could have been far worse: the 1918/19 H1N1 killed more people than both World Wars combined in a single season. It killed more people in 24 months than AIDS killed in 24 years and more in a year than the Black Death did in a century. Over a quarter of patients who caught (A)H1N1 in hospital died because of it.
So we do need to take flu seriously, but how does it compare with COVID?
| Influenza Virus | SARS-CoV-2 | |
|---|---|---|
| Individual Level | ||
| Symptom Severity | Flu usually presents as a sudden onset of fever, chills, muscle aches, fatigue, headache, and cough. While flu can lead to severe outcomes (such as pneumonia or hospitalisation), the majority of cases are mild to moderate, especially in healthy individuals. |
COVID presentations can range from mild to severe, and symptoms can include fever, cough, fatigue, loss of taste or smell, shortness of breath, and in severe cases difficulty breathing. COVID also has a more varied course; some people experience mild symptoms while others – especially the elderly or those with pre-existing conditions – may develop severe illness, including acute respiratory distress, organ failure, even death. |
| Mortality Rate | The case fatality rate (CFR) for seasonal flu is typically low, with estimates between 0.1% and 0.2%, depending on the population. It’s rarely fatal in the otherwise healthy, but complications can arise in vulnerable groups such as young children, the elderly, the immunocompromised. |
The CFR for COVID varies significantly, depending on age, underlying conditions and access to healthcare. It is generally higher than for seasonal flu, with early estimates around 1-2% globally, though this varies. COVID-19 is more likely to cause severe illness in vulnerable populations. |
| Long-Term Effects | Long-term complications from the flu are rare. Severe cases may lead to prolonged recovery times, especially in those with pre-existing health conditions. | COVID is associated with ‘Long COVID’ – fatigue, brain fog, shortness of breath – for months after the initial infection, even if the case was mild. Organ damage and long-term cardiovascular / respiratory problems can also occur in severe cases. |
| Population Level | ||
| Transmission | Flu spreads quickly through respiratory droplets and has a basic reproduction number (R0) of 1.3, meaning each infected person typically infects 1-2 others. Flu spreads seasonally, with yearly waves typically peaking in winter months. |
COVID spreads more easily than the flu, with an R0 estimated between 2-3 for the original strain, though newer variants like Delta or Omicron were more contagious (8 or higher). Unlike flu, SARS-CoV-2 also spreads asymptomatically, making control more challenging. |
| Immunity | There is a degree of pre-existing immunity in the population due to prior infections and annual vaccinations. Flu vaccines are updated yearly to reflect circulating strains, but because production takes several months, each annual vaccine offers varying levels of protection depending how closely it matches the strains circulating during the winter. |
There was no pre-existing immunity when SARS-CoV-2 first emerged. Antibodies (whether from infection or vaccination) wane over time, and new variants can escape antibodies to varying extents, but protection remains good against severe illness. mRNA vaccines can be put into production far more quickly than flu vaccines. |
| Healthcare Impact | A severe flu season can strain healthcare systems but usually does not overwhelm them in countries with robust infrastructure. Hospitalisation rates tend to be predictable based on seasonal patterns. |
COVID placed unprecedented strains on healthcare systems worldwide, particularly during surges. High hospitalisation rates and ICU occupancy and the need for ventilators overwhelmed resources. This led to healthcare rationing in some areas, especially during early waves before therapeutic drugs and vaccines were widely available. |
| Mortality | Seasonal flu causes between 290,000 to 650,000 respiratory deaths globally each year. While these numbers are significant, they are far lower than the deaths caused by COVID. |
COVID has caused millions of deaths worldwide since the start of the pandemic. It’s not just deaths directly attributable to COVID: lockdown led to – amongst other issues – underdiagnosis of cancer and other life-threatening conditions. |
However there was legitimate fear and uncertainty and many conflicting messages. And nature abhors a vacuum: in the absence of reliable and concise information, something needs to fill the gap. The myths that circulated alongside the virus included:
- The virus was a hoax / it was planned by Governments or unnamed bad actors.
- It was spread by 5G networks somehow activating bats. Or something.
- Vaccines contained microchip / nanobot tracking devices – which people would furiously tweet about using the tracking device they had been carrying in their pocket for years.
- The virus was engineered to target certain ethnic groups (or not target others).
But some fears were legitimate and we’ve covered some of the more sensible questions / fears below.
Can mRNA vaccines ‘reprogramme’ our DNA?
No. That’s not possible. If RNA vaccines could change DNA we would have a whole new world of genetic medicine.
Also the DNA in your cells is in the nucleus, surrounded by a double membrane that blocks the entry of large molecules like spike mRNA. Even if the vaccine RNA could enter the nucleus (it can’t), it would then need the enzymes to convert it back into DNA (reverse transcriptases) and to insinuate it into our genome (integrases). Some viruses can do that (retroviruses such as HIV, for example) but coronaviruses can’t.
Only about 4% of our DNA codes for functional proteins, while 8% consists of retroviral DNA that has been embedded in our genome ever since some retrovirus or other infected one of our ancestors millions of years ago.
For example, syncytin started as a retroviral envelope protein, now it allows the placenta to develop by fusing cells together during foetal development. Without this retroviral gene, mammals (including humans) would still be laying eggs.
Do vaccinated people shed virus?
There is no virus in the vaccine. You can’t get COVID from the vaccine so you can’t ‘shed’ it.
Is ‘natural’ immunity better?
While it’s true that getting infected will give you a degree of immunity, it’s less predictable. And you bear all the risks that come with a COVID infection: the possibility of severe illness and death, Long COVID and long term cognitive decline. These are not associated with vaccination.
Some argue that the vaccine is somehow ‘more dangerous’ than actually getting COVID. If we round the numbers a bit there were about 250,000 deaths associated with about 25,000,000 cases in the UK. So let’s say COVID has a 1% mortality rate. Yes, it was higher early on, and some groups were more likely to experience worse outcomes.
If we take out the very young and the unvaccinated from the population, this means at least 50 million people have been vaccinated in the UK. So for the vaccine to be more deadly than the disease, more than half a million people would have died after vaccination. We reckon someone might have noticed that.
Surely waiting for natural herd immunity would have been safer?
This was always a myth. There is no such thing as ‘natural’ herd immunity from letting people get infected.
This idea was proposed by some politicians and economists early on who called for ‘focused protection‘ for the elderly and vulnerable, to allow the rest of society to return to normal life and build up herd immunity. This may sound plausible – but it’s self-evidently unviable.
Were that approach effective, we would have developed herd immunity to smallpox and countless other diseases that have plagued us since antiquity aeons ago. Population immunity (to give it its proper title) can only happen when an entire population is vaccinated – but even then new, susceptible hosts will continue to be born.
We already operate a form of ‘focused protection’ for seasonal flu in the UK – we vaccinate the elderly and vulnerable, and also those that may spread it to them – children. And if they do get it we have zanamivir, oseltamivir and other antivirals. But when the ‘let it rip’ herd immunity strategy was proposed, we had neither vaccines nor therapeutics for COVID-19. It would have been a disaster.
The proportion of the community you need to vaccinate to achieve herd immunity varies; it can be as low as 50% but this is rare. It’s usually more like 90%, especially for something really contagious.
In fact, you can calculate the herd immunity ‘threshold’: it’s (R0 − 1)/R0. Remember R0? That’s the basic reproduction number – how many people someone with it is likely to pass it on to. So for measlesR0 is 18, so (18-1)/18 = 94% (measles is remarkably contagious) but for something with R0 = 4 you’d need at least 75% vaccinated.
For eradication there needs to be no animal reservoir as well. We were only able to eradicate smallpox by vaccinating the world, and due to there being no animal reservoir that it could spill over from again. It’s the same with poliovirus: we were close to eradicating polio (and may well still manage it) through vaccination – because there is no animal reservoir for it to bounce back from. When it’s gone, it’s gone.
Even if we were able to persuade everyone to slow the spread of a fatal disease by engaging in behaviours such as masking and getting vaccinated (which means making vaccines globally available too) there are still animal reservoirs and intermediate hosts for coronaviruses to jump from.
But what about Sweden?
Many have claimed that Sweden was a pandemic paradise, which neither imposed restrictions on its citizens nor closed schools. This is a myth. In fact, Sweden took drastic measures to control the virus at times – travel restrictions, school closures, venue closures – but too late for many of its most vulnerable citizens.
Early on, Stockholm’s nursing homes ended up losing about 7% of their 14,000 residents to the virus. About 1,000 died in a matter of weeks. The vast majority were not taken to hospitals. Many of the elderly were given morphine instead of oxygen despite supplies being available, effectively ending their lives. You can see the effect compared with neighbouring countries here:
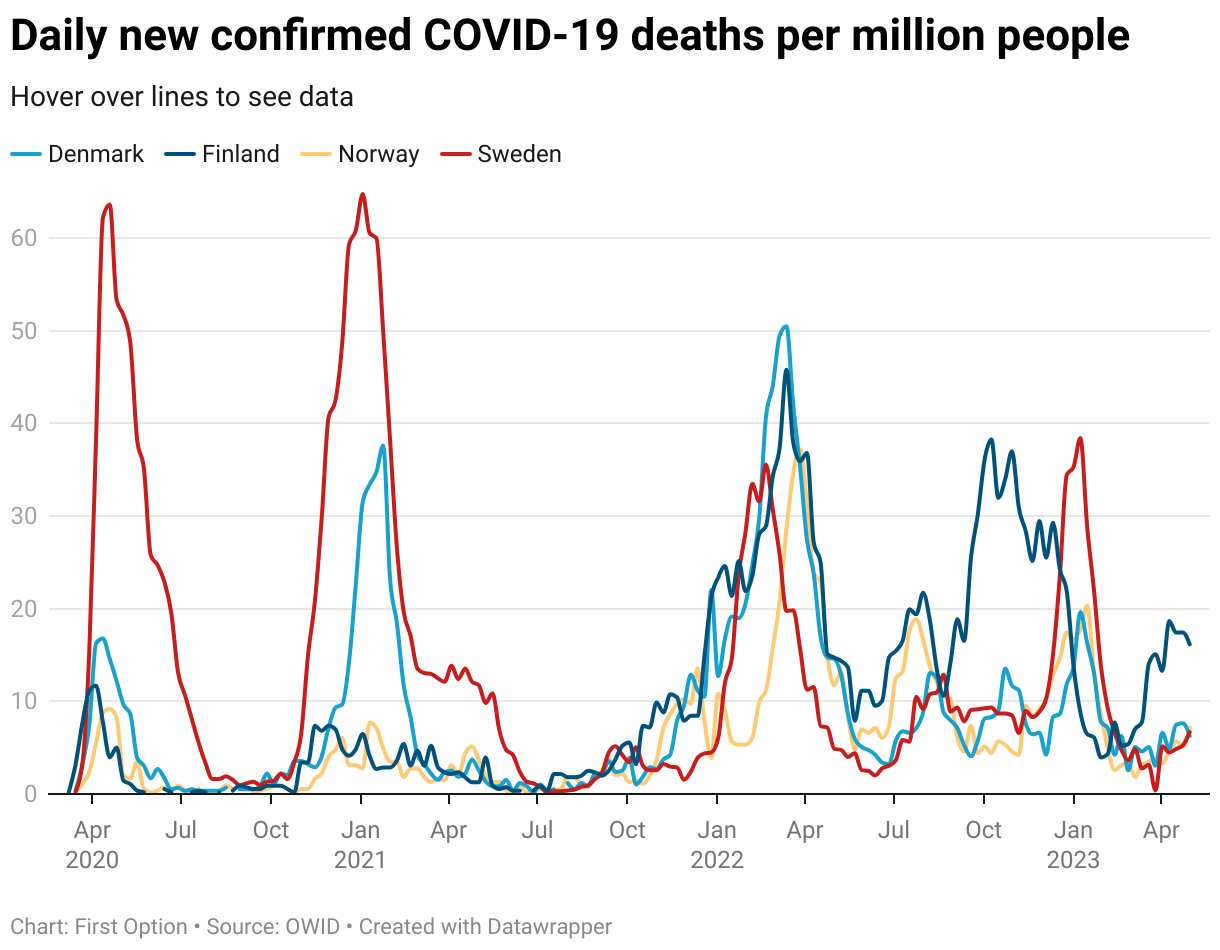
You can see the two huge early peaks in deaths for Sweden, thereafter it tracks well with neighbouring countries. Their approach will be a topic of discussion for years to come, but any claims that they did nothing to control the virus or that their initial hesitation came without consequences are very wide of the mark.
Some have pivoted the argument to “now their excess mortality rates are the lowest in Scandinavia“. This is because they sacrificed the elderly and vulnerable early on – and people can’t die twice and get counted in mortality figures twice.
But most of the people in hospital are vaccinated?
This is an example of Base Rate Bias. Think about it: if 100% of the population is vaccinated, 100% of the cases will be in the vaccinated. There will always be vaccinated people ending up in hospital.
Or to put it another way, if you have a village of 100 people where 99 are vaccinated and you get two cases (one in a vaccinated person) then yes, 50% of cases will be in the vaccinated. But that’s looking at it the wrong way. A more illustrative way or representing this is that 1% of the vaccinated and 100% of the unvaccinated became infected.
What about…
It’s also a myth that any of the vaccines caused infertility, were developed too fast or caused spontaneous miscarriage .
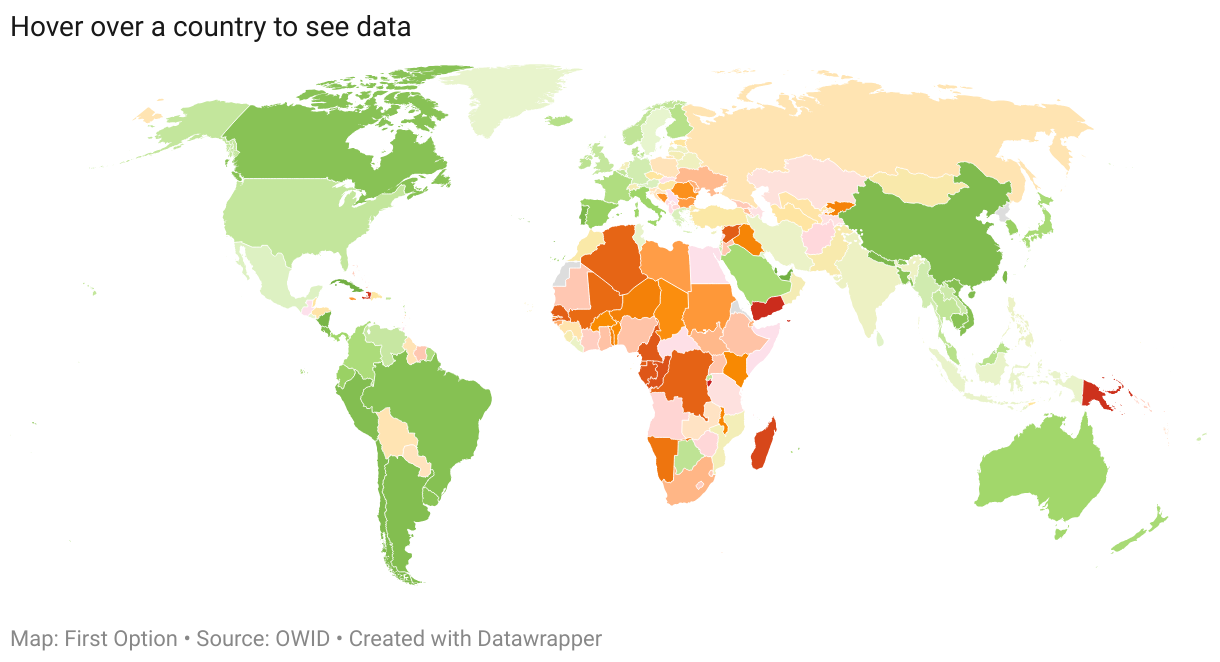
COVID in Maps
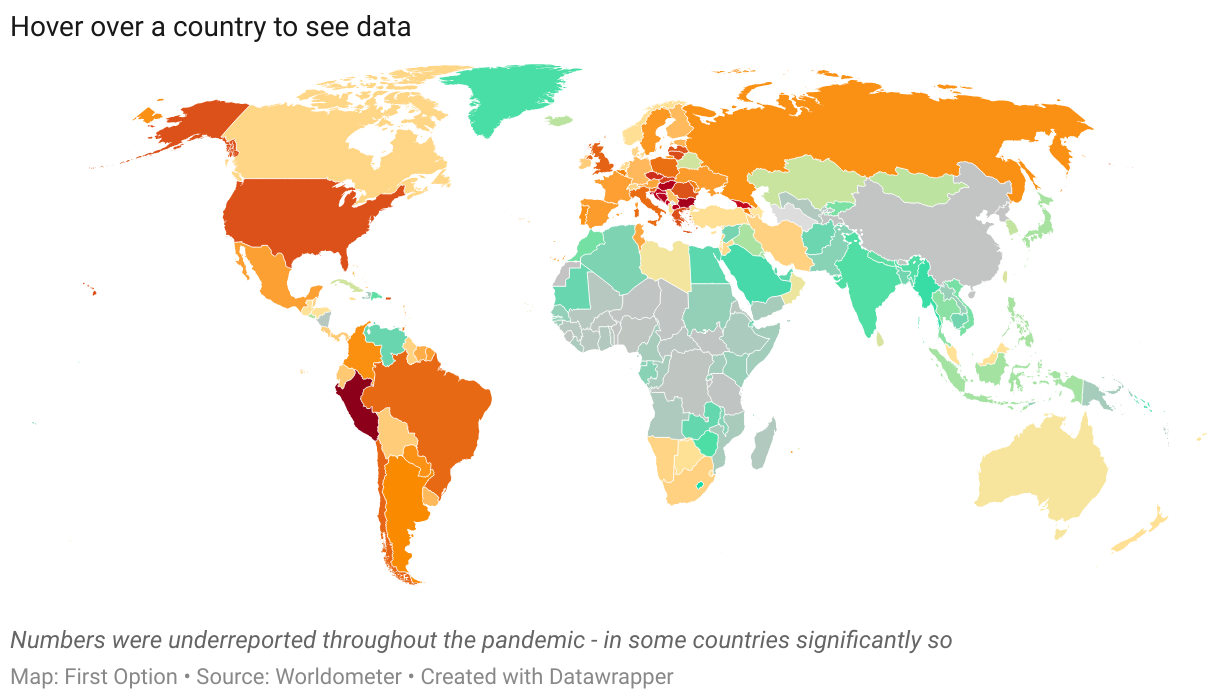
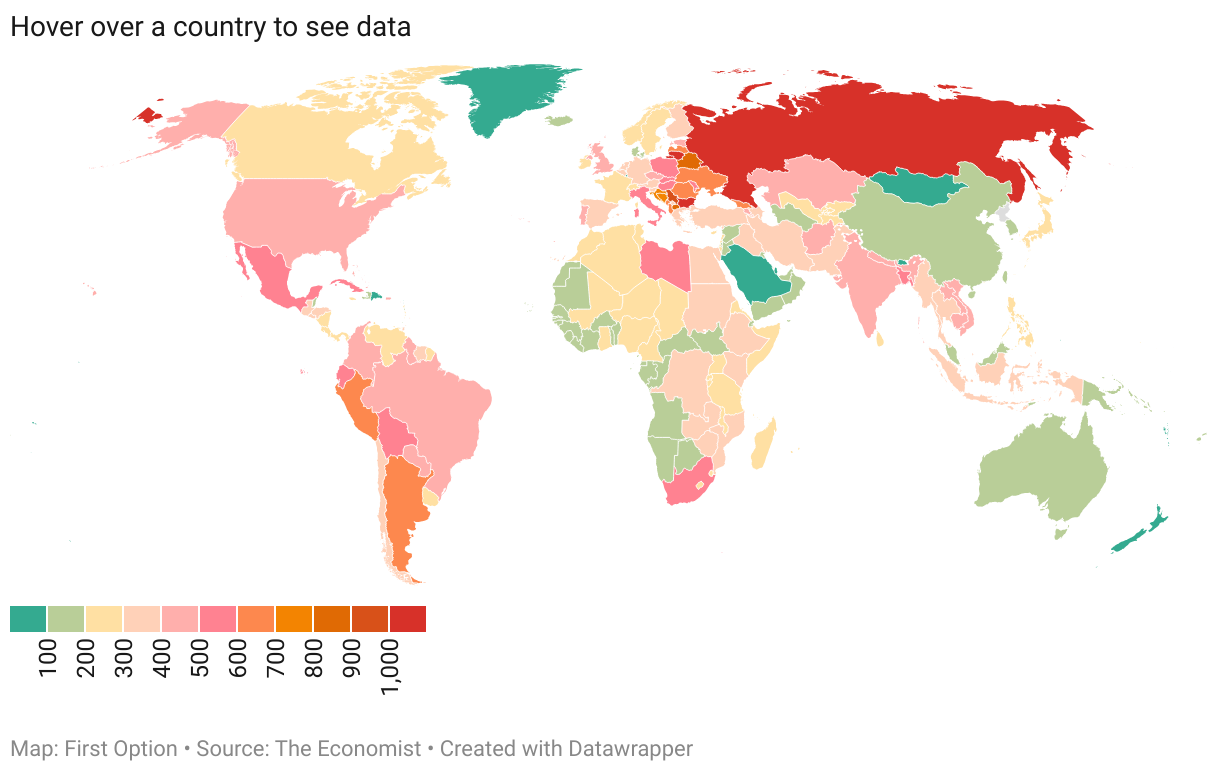
7,014
Article last updated on Oct 2nd, 2025


