





Influenza
Influenza is a contagious seasonal virus that affects 5 – 10% of adults and 20 – 30% of children every year, killing an average of 700,000 people worldwide.
It kills directly through viral pneumonia but also kills indirectly by making other conditions worse, via secondary bacterial infections, and thrombotic events such as heart attacks and strokes.
However, the risk of dying from influenza has declined substantially over time due to improved treatments, sanitation, and vaccination. We might be used to ‘living with‘ flu but its potential impact on productions should not be underestimated. Fortunately some simple precautions can help reduce the risk.
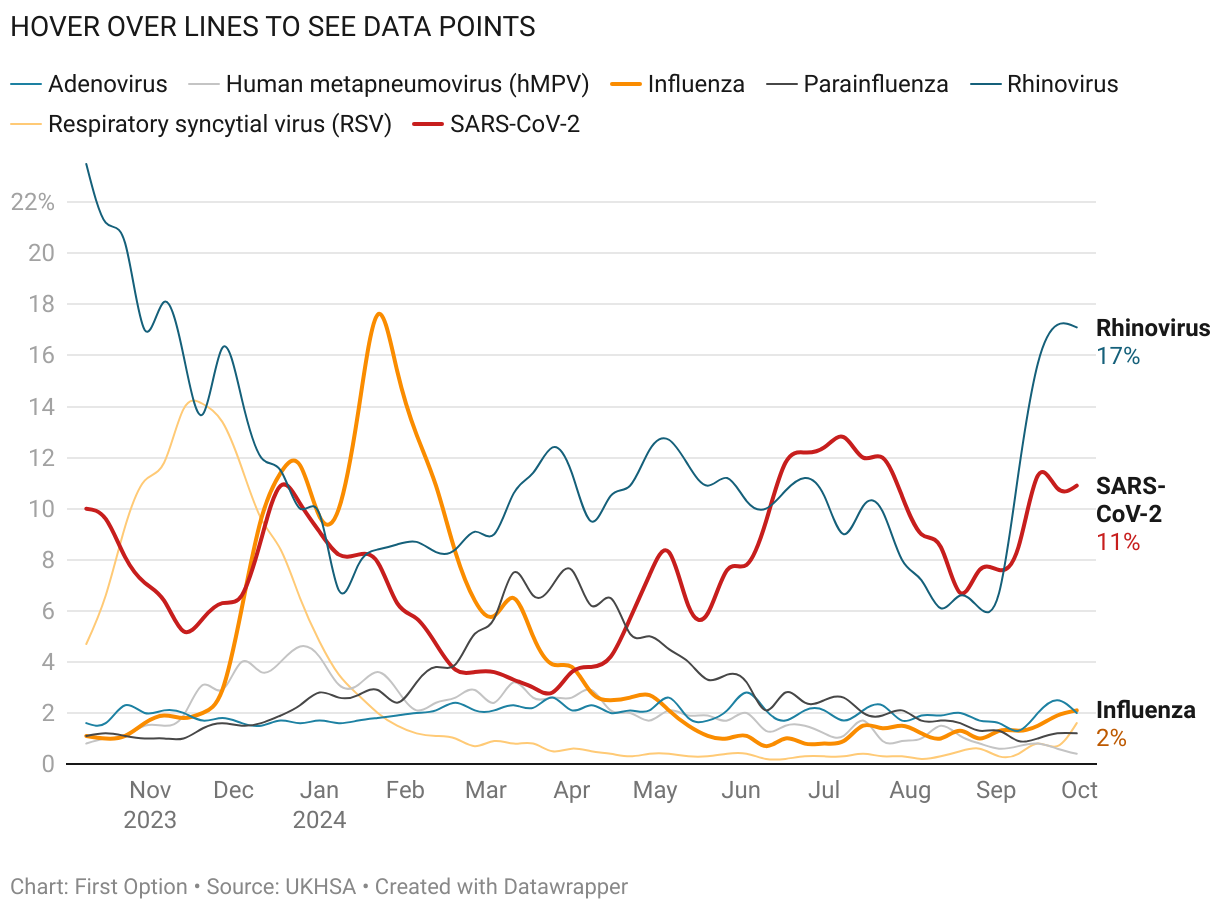
Respiratory Virus Snapshot
FLU
MEDIUM | Activity IncreasingInfluenza Virus
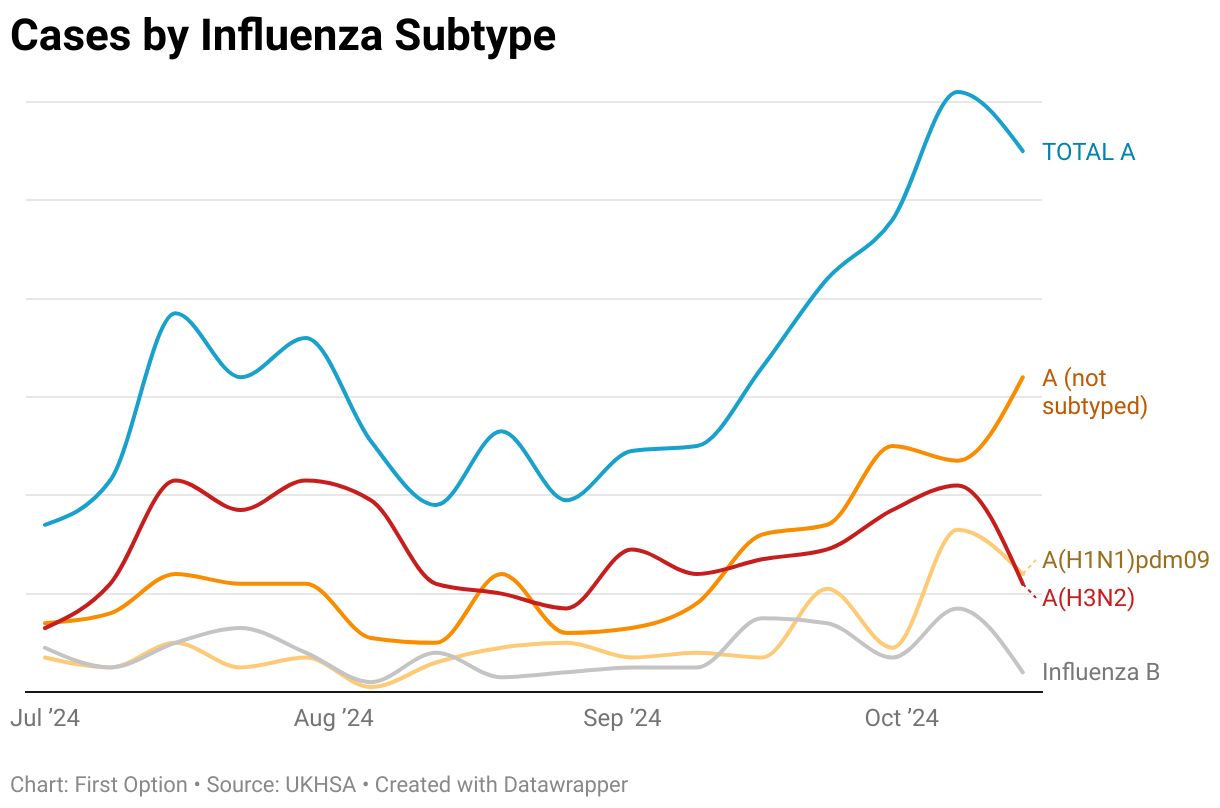
Influenza activity is circulating at medium levels and increasing. Emergency department (ED) attendances for influenza-like-illness (ILI) rising as well asinfluenza-confirmed acute respiratory infections (ARI). Of influenza viruses subtyped, the majority were A(H3N2).
COVID
MIXED | Circulating at baseline levelsSARS-CoV-2
Activity showing mixed trends. ED attendances for COVID-19-like illness remains stable. Reported SARS-CoV-2-confirmed acute respiratory infections (ARI) remain stable week-on-week.
RSV
MEDIUM | Mixed activity across indicators, circulating at medium levelsRespiratory Syncytial Virus
RSV activity showed mixed trends across indicators and is circulating at medium levels. ED attendances for acute bronchiolitis increasing.
Updated 3rd January, 2026
Influenza | Key Facts
Seasonal Flu: Advice to Productions
Where is your risk?
A ‘proper’ flu infection (as opposed to colds) will likely make someone sick enough not to be able to work so you should consider the impact of someone having to take time off sick. For example, if you have talent who may need to take time off how will that impact your production as this could pose a potentially significant business continuity risk.
- Who are the key people that are critical to the production staying disruption-free? What can you do to keep them from (a) getting it and (b) coming into contact with anyone who may be infected?
- While flu is not as contagious as SARS-CoV-2, identify those who could spread the virus if they become infected. It’s not just cast members or contributors, it’s those working in close proximity too: HMU, costume, unit drivers etc.
Beyond business risk, your highest risk is likely to involve vulnerable persons. These are individuals who, were they to contract the virus, could be at a higher risk to their health due to their individual circumstances. Age and pre-existing health conditions (especially respiratory) are the key factors to consider.
You will need to assess the work activity based on the personal circumstances of these individuals on a case-by-case basis and decide whether additional measures are appropriate to reduce their risks to an acceptable level.
Control Measures for Consideration
Vaccination
Vaccination reduces the risk of severe illness, hospitalisation and death. But while vaccination can reduce the risk of transmission and infection, it doesn’t eliminate it. The flu vaccine is a bit of an annual lottery – see below – but just because it is not 100% protective, that doesn’t make it 100% worthless. That’s a false binary.
Ventilation
Make sure that your workplace is well ventilated and do all you can to keep a regular supply of fresh air passing through either through general ventilation or air conditioning. Where you identify poorly ventilated areas in certain indoor locations a specific assessment might be needed. The infection risk may be higher in areas where you cannot easily use general ventilation (utilising open doors and windows) and so you may be reliant on recirculating air conditioning and other mechanical systems.
Face Coverings and Masks
The wearing of face masks is not popular post-COVID but there may be certain circumstances whereby it is still prudent to consider their use.
Where the risk or consequence of transmission is high and other safety measures are not available, the use of masks should be considered. For example this may include when working in close contact or with vulnerable individuals.
Isolate When Sick
When employees are ill, you should look to encourage them to avoid coming into work. This prevents an infectious person potentially spreading the virus to others in the workplace. In instances whereby it cannot be avoided that a sick person attends (such as required talent) you should assess their workplace to ensure the protection of others. That may include introducing social distancing measures and requiring mask wearing, use of screens and back to back/side to side seating as examples.
Testing
Lateral flow tests that can detect influenza viral antigens in 10-15 minutes are available, but they only have moderate sensitivity so will only correctly identify a positive 50-70% of the time. They do have high specificity so false positives are unlikely.
Our view is that testing is of limited utility: the incubation time is short and system onset is rapid so people are likely to feel dreadful quite quickly. But if someone absolutely has to battle on during an infection, knowing that they have flu (or COVID) rather than something less serious – especially if working in close contact with higher risk individuals – might help inform your containment strategy.
Cleaning
Regular general cleaning is still an effective way to protect against any number of other viruses. This should take into account the amount and type of usage that an area has.
It is unlikely that fogging or deep cleans, or regular cleaning of touch points throughout the day will continue to be appropriate or practicable. You may want to look at different options such as providing wipes for wiping down of hot desks and equipment for individuals to utilise before use.
However, daily general cleaning is likely to be sufficient in most circumstances.
Hygiene
Remind people that practising good hygiene continues to play an important part of preventing spread of disease. Look to ensure that the workforce’s access to welfare facilities is appropriate and where necessary look to provide suitable alternatives such as hand gels and wipes.
Hand washing is always preferable to hand gels, and good respiratory hygiene (coughing or sneezing into a tissue or your sleeve) is important to help stop the spread of flu and other seasonal ILIs.
Vaccines
A new flu vaccine is required every year for a number of reasons. There’s the constant genetic drift of the virus. Also different strains rise and fall over time – in fact the Influenza B Yamagata strain seems to have become extinct over lockdown: it seems it simply ran out of hosts when people weren’t mixing and passing it on.
This challenge is exacerbated by the way flu vaccines have been produced since the 1940s: each dose is grown in a hen’s egg. This takes time.
- The WHO makes recommendations on the composition of the northern hemisphere flu vaccine each February. Their recommendations are based on the flu virus strains that they judge to be the most likely to circulate the following winter, and take into account data from the southern hemisphere flu season.
- Production of the vaccine usually runs from March to August / September, and packaging and labelling can continue until October.
- Once vaccine composition is agreed, then the manufacturers have to grow the vaccine viruses, formulate the vaccine, test, license, and package and supply the vaccine within six months in order to ensure stocks are available in time. Most manufacturers then immediately switch to flu vaccine production for the next southern hemisphere season. Hence, the flu vaccine production period is limited and complex, with little room for slippage in the process.
However, advances in cell culture technology and genetic engineering mean that faster techniques are now coming on line with shorter lead times – and a combined mRNA combined flu / COVID shot may be available as early as 2026. It is hoped mRNA vaccines will be faster to make and update than the current ones used against flu, and be a better match for ever-changing strains.
How protective is the vaccine?
It varies from season to season. Because of the mutation rate and the lead time for the vaccine, it’s more protective in some years than others. But protection against mild disease will always be partial – the incubation period is far shorter than the time it takes for the immune system to mount specific defences against the virus.
This is true of all vaccines against viruses with short incubation periods such as flu and COVID; they are more protective against severe disease. In these cases, vaccines act like fire extinguishers – they won’t prevent a fire in your kitchen but they will stop it before the house burns down.
Impact of Seasonal Flu
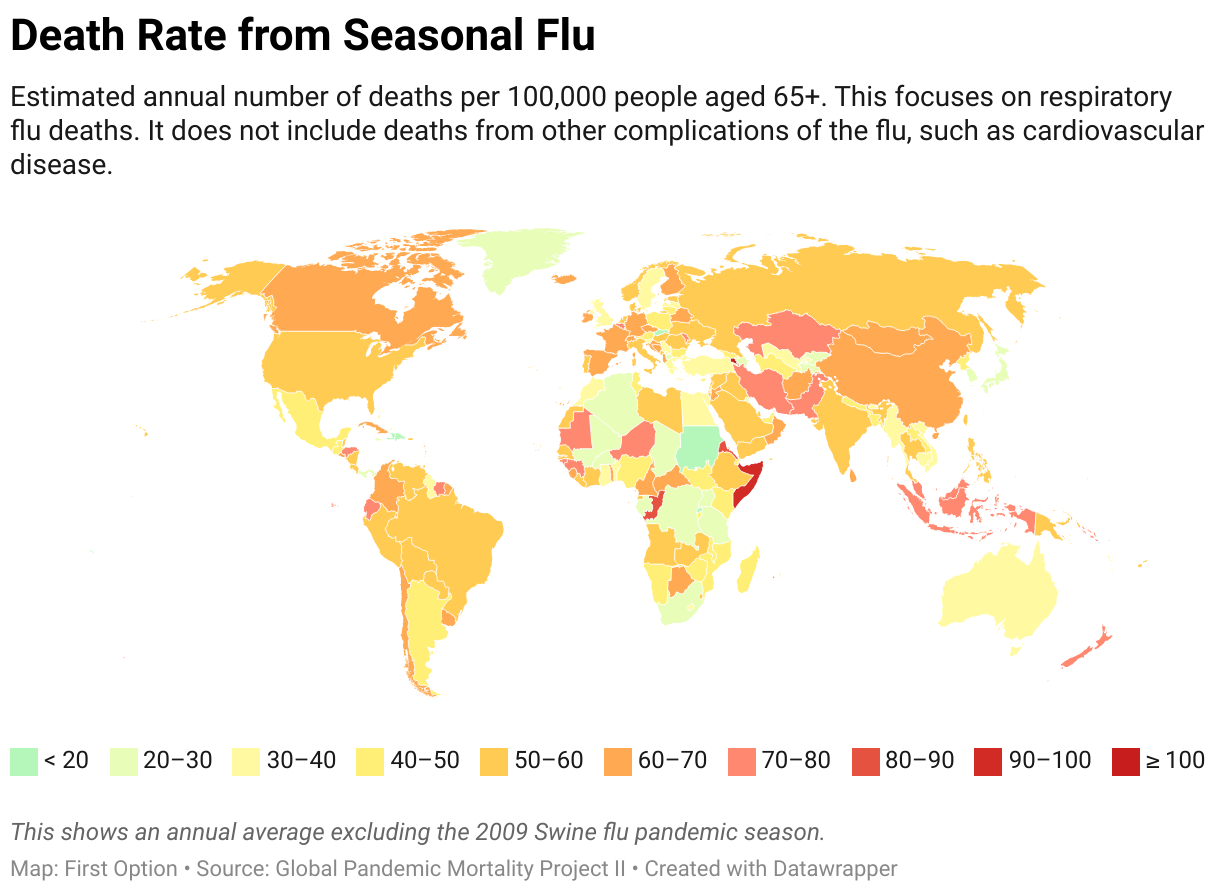
Influenza rolls around the world in seasonal epidemics, resulting in countless millions of cases and hundreds of thousands of deaths every year. Human influenza has two main types: A and B (there is a C too), and in any season there are generally two A strains and one B in circulation. Influenza B is less common, less virulent and has a slower mutation rate – which makes it less of a risk than A strains.
Different strains have different virulence (ability to cause disease) and different infectivity (ability to spread). Some pandemics such as the 1919 H1N1 were both virulent and infective and killed around 5% of the world’s population – or more than both World Wars combined.
Influenza kills, especially in the young, the old, the obese and the pregnant. It kills directly, it kills by acute secondary infections, it kills by worsening underlying diseases like heart failure, and it kills long-term by increasing vascular events like heart attack and stroke.
Deaths caused by influenza also depend on the virulence of the circulating strains. Some strains such as H5N1 or H3N2 are more likely to kill (60% for H5N1) than strains such as H1N1 which has been of only moderate virulence – but very infectious.
Influenza deaths, both direct and indirect, are difficult to measure and are at best an estimate. As an example somewhere between 150,000 to 600,000 people died worldwide in the 2009 H1N1 swine flu pandemic (on top of seasonal flu deaths), with a mean estimate of about 250,000.
Flu vs COVID
The influenza virus and SARS-CoV-2 have some superficial similarities. Both spread in a similar way. Both have RNA as their genetic material. Both present initially with similar symptoms. But despite these similarities they are very different in terms of their effects at both individual and population level.
To summarise, COVID is a lot worse on every level – but don’t underestimate flu. It preferentially kills the old, the young, the infirm, the obese and the pregnant, but it kills the healthy too by making other conditions worse and killing indirectly via acute secondary infections, increasing risk of vascular events like stroke and heart attack and by worsening underlying diseases like congestive heart failure and chronic bronchitis.
The 1918/19 H1N1 killed more people than both World Wars combined in a single season, it killed more people in 24 months than AIDS killed in 24 years and more in a year than the Black Death did in a century.
So we do need to take flu seriously, but how do the two compare?
| Influenza Virus | SARS-CoV-2 | |
|---|---|---|
| Individual Level | ||
| Symptom Severity | Flu usually presents as a sudden onset of fever, chills, muscle aches, fatigue, headache, and cough. While flu can lead to severe outcomes (such as pneumonia or hospitalisation), the majority of cases are mild to moderate, especially in healthy individuals. |
COVID presentations can range from mild to severe, and symptoms can include fever, cough, fatigue, loss of taste or smell, shortness of breath, and in severe cases difficulty breathing. COVID also has a more varied course; some people experience mild symptoms while others – especially the elderly or those with pre-existing conditions – may develop severe illness, including acute respiratory distress, organ failure, even death. |
| Mortality Rate | The case fatality rate (CFR) for seasonal flu is typically low, with estimates between 0.1% and 0.2%, depending on the population. It’s rarely fatal in the otherwise healthy, but complications can arise in vulnerable groups such as young children, the elderly, the immunocompromised. |
The CFR for COVID varies significantly, depending on age, underlying conditions and access to healthcare. It is generally higher than for seasonal flu, with early estimates around 1-2% globally, though this varies. COVID-19 is more likely to cause severe illness in vulnerable populations. |
| Long-Term Effects | Long-term complications from the flu are rare. Severe cases may lead to prolonged recovery times, especially in those with pre-existing health conditions. | COVID is associated with ‘Long COVID’ – fatigue, brain fog, shortness of breath – for months after the initial infection, even if the case was mild. Organ damage and long-term cardiovascular / respiratory problems can also occur in severe cases. |
| Population Level | ||
| Transmission | Flu spreads quickly through respiratory droplets and has a basic reproduction number (R0) of 1.3, meaning each infected person typically infects 1-2 others. Flu spreads seasonally, with yearly waves typically peaking in winter months. |
COVID spreads more easily than the flu, with an R0 estimated between 2-3 for the original strain, though newer variants like Delta or Omicron were more contagious (8 or higher). Unlike flu, SARS-CoV-2 also spreads asymptomatically, making control more challenging. |
| Immunity | There is a degree of pre-existing immunity in the population due to prior infections and annual vaccinations. Flu vaccines are updated yearly to reflect circulating strains, but because production takes several months, each annual vaccine offers varying levels of protection depending how closely it matches the strains circulating during the winter. |
There was no pre-existing immunity when SARS-CoV-2 first emerged. Antibodies (whether from infection or vaccination) wane over time, and new variants can escape antibodies to varying extents, but protection remains good against severe illness. mRNA vaccines can be put into production far more quickly than flu vaccines. |
| Healthcare Impact | A severe flu season can strain healthcare systems but usually does not overwhelm them in countries with robust infrastructure. Hospitalisation rates tend to be predictable based on seasonal patterns. |
COVID placed unprecedented strains on healthcare systems worldwide, particularly during surges. High hospitalisation rates and ICU occupancy and the need for ventilators overwhelmed resources. This led to healthcare rationing in some areas, especially during early waves before therapeutic drugs and vaccines were widely available. |
| Mortality | Seasonal flu causes between 290,000 to 650,000 respiratory deaths globally each year. While these numbers are significant, they are far lower than the deaths caused by COVID. |
COVID has caused millions of deaths worldwide since the start of the pandemic. It’s not just deaths directly attributable to COVID: lockdown led to – amongst other issues – underdiagnosis of cancer and other life-threatening conditions. |
Flu Strains
The seriousness of flu depends in part on the virulence of the circulating strains. Some strains, such as H5N1 (bird flu) or H3N2, are more likely to kill (60% for H5N1) than strains like H1N1 which was of only moderate virulence but highly infective.
The ‘H’ and ‘N’ refer to slightly different forms of molecules called haemagglutinin and neuraminidase.
Haemagglutinin enables flu virus to bind to and enter a host cell. Neuraminidase helps daughter viruses break out of an infected cell to infect another. Drugs such as Oseltamivir (Tamiflu) are neuraminidase inhibitors and so limit the severity of a flu infection.
There are many different types of flu. Human flu. Bird flu. Horse flu. Swine flu. By and large, different types stick to their host species, but flu is one of those rare viruses that can jump across species if it has a mind to. So, a pig can be infected by both bird flu and human flu – as well as swine flu. But as a rule humans get flu from humans, not birds or pigs.
This is where it gets interesting. The flu virus keeps its genetic material of just 11 genes in 8 different segments or ‘packets’ rather than as a single unit. Unlike our DNA, the RNA of influenza replicates without the benefit of enzymes that correct copying errors. This makes replication sloppy, with a lot of errors – flu has one of the highest mutation rates known.
Some of these errors are neutral and have no effect on the virus. Most are detrimental and will result in a defective virus. But some of them will make it more infective or more virulent.
Genetic Drift and Shift
These mutations build up during each flu season. This is called genetic drift and means the flu virus at the end of the season is slightly different to what it was at the beginning.
But because of the way flu’s genetic material is organised into segments, and because viruses are inherently sloppy in the way they reproduce, you might suddenly get a strain arise that combines elements of human, bird and swine flu viruses and – hey presto – a new strain is born.
This mainly happens in pigs, who can become infected with human flu
This is called genetic shift. And if the new strain is both virulent and infective we are in trouble.
Zoonotic Flu
Animal influenza viruses are distinct from the seasonal flu viruses that infect humans and rarely spread between people. However, zoonotic influenza viruses – those originating in animals – may occasionally infect humans and can cause a range of illness, from mild symptoms to severe disease, and even death.
Birds are natural hosts of avian flu. Following an outbreak of the A(H5N1) virus in poultry in Hong Kong in 1997, avian flu strains, including A(H5N1), have spread from Asia to Europe and Africa since 2003. In 2013, cases of human infection with the A(H7N9) strain were also reported in China.
Most swine flu viruses don’t normally infect humans, but some countries have reported cases where people were infected. These cases often involved close contact with infected pigs, though in rare instances, human-to-human transmission has been observed.
H1N1
The 1919 H1N1 killed ~ 5% of the world’s population, by comparison 90 years later the 2009 H1N1 was highly infectious but not particularly virulent. The 2009 H1N1 had a mortality rate of 0.6%, and since that number is based on hospitalised cases, the true death rate is probably lower.
Genetic analyses of this virus have shown that it originated from animal influenza viruses and is unrelated to the human seasonal H1N1 viruses that have been in general circulation among people since 1977. It is still included in annual vaccines.
The groups most at risk of dying from H1N1 are those less than 60 and healthy. This sounds somewhat counterintuitive, but in part this H1N1 can be traced back to the 1918 strain and explains why those over 60 have a decreased death rate rather than the usual increased mortality from influenza: old people have cross-reacting antibodies to the strain that is protective.
This strain is only new to people born since around 1950, so billions of people at risk due to lack of immunity. But as far as virulence and antigenicity, it is the same old flu, re-assorting its RNA to come up with new strains as it has always done and will continue to do as long as there are people pigs and birds around to get influenza.
H5N1
Influenza A virus subtype H5N1 – Bird Flu – is very virulent but not very infective. H7N9 seems to have a similar profile. This is because the receptor molecules that the virus can bind to (in order to start the process of infecting us) are found deep in our lungs. To catch it you need to be around a lot of infected poultry and breathe very deeply.
Can humans get bird flu?
Yes. But infrequently. This is all about where the receptors the flu virus binds to are to be found.
The H1N1 receptors are in the upper airway so it’s far more infective in humans. This makes H1N1 far more infective but fortunately it’s far less virulent. Avian influenza strains preferentially bind to alpha (2,3) sialic acids – the major sialic acid on epithelial cells of the duck gut. In contrast, human influenza virus strains preferentially attach to alpha (2,6) sialic acids – the major type of sialic acid present on human respiratory epithelial cells. We do have alpha (2,3) sialic acids but as above these found in the lower respiratory tract.
So, efficient human to human transmission requires strains that like binding to (2,6) sialic acids and tests on influenza virus isolates from the 1918, 1957, and 1968 pandemics suggest that those flu viruses preferentially recognised alpha (2,6) linked sialic acids.
Epithelial cells of the pig trachea produce both alpha (2,3) and alpha (2,6) linked sialic acids. This is believed to be the reason why pigs can be infected with both avian and human influenza virus strains and serve as a ‘mixing vessel’ for the emergence of new viruses.
Haemagglutinins
As mentioned above, the haemagglutinin protein on the flu virus coat help it get into a human cell to start the process of infection and replication. You can see below which animals have receptors for the 18 different haemagglutinins. you can see the commonality among humans, birds and pigs clearly.
| Subtype | People | Birds | Swine | Bats | Cats | Dogs | Horses | Cows |
|---|---|---|---|---|---|---|---|---|
| H1 | ||||||||
| H2 | ||||||||
| H3 | ||||||||
| H4 | ||||||||
| H5 | ||||||||
| H6 | ||||||||
| H7 | ||||||||
| H8 | ||||||||
| H9 | ||||||||
| H10 | ||||||||
| H11 | ||||||||
| H12 | ||||||||
| H13 | ||||||||
| H14 | ||||||||
| H15 | ||||||||
| H16 | ||||||||
| H17 | ||||||||
| H18 |
Neuraminidases
The virus needs a haemagglutinin to get into a cell, it’s the neuraminidase helps it get out again.
| Subtype | People | Birds | Swine | Bats | Cats | Dogs | Horses | Cows |
|---|---|---|---|---|---|---|---|---|
| N1 | ||||||||
| N2 | ||||||||
| N3 | ||||||||
| N4 | ||||||||
| N5 | ||||||||
| N6 | ||||||||
| N7 | ||||||||
| N8 | ||||||||
| N9 | ||||||||
| N10 | ||||||||
| N11 |
You can work out from the above where there is a possibility of transfer between species but a match above does not guarantee transmissibility.
Canine influenza (dog flu) is caused by an A(H3N2) that spreads in dogs but poses a low threat to people. This is because canine influenza A(H3N2) viruses are slightly different to the seasonal influenza A(H3N2) that spreads among people. To date there is no evidence of spread of canine influenza viruses from dogs to people.
The only combination that could pass between horses and dogs is H3N8 and there have been isolated incidences in the UK, South Korea, China, Thailand, the USA and Canada.
Note that while humans do have receptors for (say) H5, most flu viruses that infect humans are H1, H2 and H3.
3,353
Article last updated on Jan 3rd, 2026


