





Marburg Virus
Marburg virus (MARV), the causative agent for Marburg Virus Disease (MVD), is a highly pathogenic RNA virus from the filovirus family. Although rare, MVD can lead to a rapidly progressing and often fatal viral haemorrhagic fever (VHF).
Among the filoviruses only Marburg and Ebola are known to cause disease in humans, and both are notorious for their high case fatality rates and severe clinical presentation.
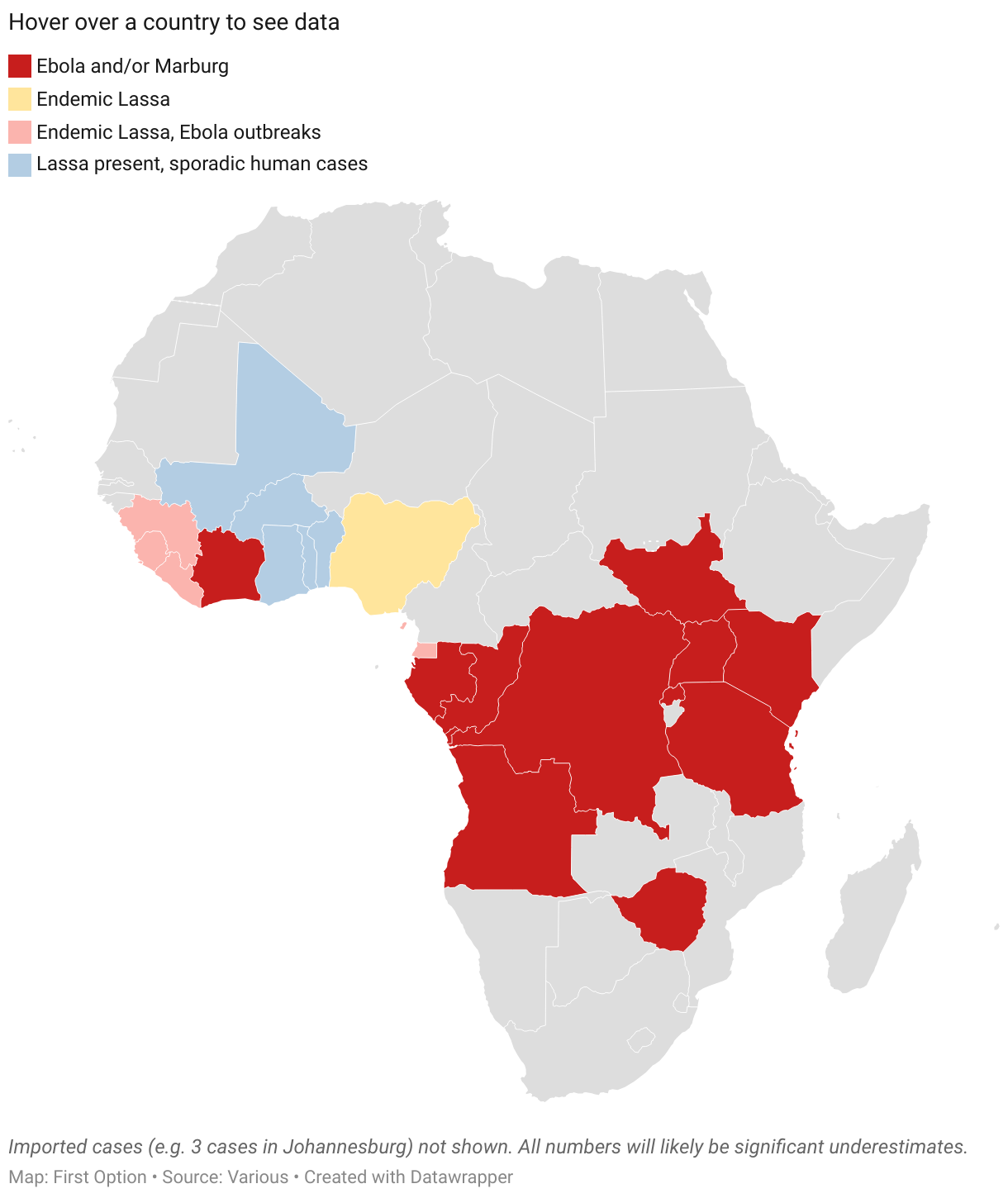
Most MVD outbreaks occur in sub-Saharan Africa, particularly in Angola, the Democratic Republic of Congo, and Uganda. However, in 2023, the US CDC issued a Health Advisory regarding the first-ever MVD outbreaks in Equatorial Guinea and Tanzania – two countries that are geographically distant and whose outbreaks were epidemiologically unrelated.
Now cases have emerged in Rwanda with most occurring among healthcare workers in the country’s capital, Kigali.
Viral Haemorrhagic Fever Hotspots
Sources and Spread
Sporadic Marburg virus outbreaks in sub-Saharan Africa are associated with high case fatality rates, usually between 80% and 90%. These outbreaks are usually linked to human exposure to oral secretions or urine and droppings from Egyptian fruit bats , the natural reservoir of the virus.
These exposures often occur among miners or tourists visiting bat-infested mines or caves, including Uganda’s Python Cave where extensive ecological studies have been conducted.
Person-to-person transmission can also occur via direct contact with the blood, faeces or bodily fluids of an infected person, or contact with contaminated objects.
Nursing someone with MVD or visiting hospitals is high risk. Traditional funerary practices and cultural factors in parts of Central Africa also aid spread. Large gatherings at funerals, open caskets and direct contact with the deceased are common, and because both Ebola and Marburg viruses remain active in the body fluids of the deceased, contact with the body can result in infection.
Risk Factors
Those travelling to affected countries are advised to avoid nonessential travel to areas with active outbreaks, and practice preventative measures including avoiding contact with sick people, blood, bodily fluids, dead bodies, fruit bats, and nonhuman primates. As ever, bushmeat should be avoided.
International travellers returning from those countries are advised to self-monitor for Marburg symptoms during travel and for 21 days after departing the area. Travellers who develop signs or symptoms of MVD should immediately self-isolate and contact their local health department / GP.
Organisations – including productions – undertaking activities in Ebola or Marburg affected areas must register with the UKHSA returning workers scheme.
Diagnosis
Clinical diagnosis of MVD is challenging because the initial ‘dry’ symptoms are non-specific (fever, influenza-like illness, malaise, anorexia) and resemble other febrile infectious illnesses. The clinical presentation is also similar to malaria, Lassa fever or typhoid, any of which the patient could have also picked up in countries where Marburg is endemic. It’s also quite possible an individual can be infected with more than one pathogen at a time.
But patients with MVD can rapidly progress from these initial nonspecific symptoms to the more severe ‘wet’ symptoms such as vomiting, diarrhoea and bleeding. Common clinical features include maculopapular rash and conjunctival suffusion early on, with most patient deaths occurring during the second week of illness progression.
Advice to Productions
Journalists and film crews traveling to affected areas must prioritise safety. This is a highly infectious virus with no cure and a high case fatality rate.
No shot – no matter how good – is worth dying for.
Despite the similarities in clinical presentation and both being filoviruses, vaccines against Ebola virus have not been shown to be protective against Marburg virus.
Pre-Travel
Medical: there is no vaccine for Marburg virus yet, but ensure you’re up-to-date on general vaccinations such as Yellow Fever, Hepatitis, and other region-specific diseases.
PPE: bring appropriate PPE such as N95 masks, gloves, goggles, and protective clothing. These will help reduce exposure, especially in high-risk zones such as hospitals.
Kit: pack a comprehensive medical kit including hand sanitisers, disinfectants, antipyretics, and first-aid supplies.
Insurance: you’ll need comprehensive medical and evacuation insurance that includes coverage for infectious disease outbreaks.
Understanding the Virus
The virus spreads through contact with body fluids (blood, vomit, saliva, faeces etc) of infected individuals, contaminated surfaces, or animals (especially fruit bats).
Incubation ranges from 2 to 21 days. Early symptoms include fever, headache, and muscle pain, but the disease can progress to haemorrhagic fever. See below.
Avoid contact with infected people, animals, or contaminated environments such as healthcare facilities.
While in the field
- Limit potential exposure: avoid hospitals and areas where infected patients are treated unless absolutely necessary. Maintain a safe distance and avoid physical contact with locals where possible.
- Interviews: use a shotgun or parabolic mic. Limit close proximity. Ensure interviewees and the crew are not exposed to high-risk environments.
- Hygiene: practice frequent handwashing with soap or use alcohol-based hand sanitizer. Avoid touching your face. Drink only bottled water and avoid eating raw or undercooked foods, especially meat.
- Stay informed: regularly update yourself on the local health situation through WHO updates or from local authorities. Outbreaks can evolve quickly and certain areas may become too risky in a short space of time.
- Emergency Evacuation Plans: establish effective communication and keep in close contact with your organisation. Have an emergency evacuation plan in place. Know where the nearest consulate or embassy is and how to access local healthcare services.
- Ethical reporting: avoid stigmatization. When reporting on an outbreak, be sensitive to how you portray affected communities. Avoid language that might stigmatise victims or spread panic.
Post Travel Health Monitoring
After returning, monitor your health for 21 days. If you experience any symptoms (fever, headache, muscle pain, etc) seek medical attention immediately and inform healthcare providers about your travel history.
Is this the ‘New COVID’?
No. Which is probably a good thing due to the utter gruesomeness of the progression of viral haemorrhagic fever infections, and their sky-high mortality rates. We don’t tend to see big VHF outbreaks for a number of reasons.
- VHFs have a high case fatality rate, so infected individuals tend to become extremely ill or die very quickly, limiting their ability to interact with others and transmit the virus on.
- VHF outbreaks are terrifying, prompting communities to rapidly adjust behaviours. Individuals avoid large gatherings and the reduce close contacts and physical interactions VHFs need to enable transmission.
- Outbreaks generally emerge in areas close to bat populations, which will be rural or isolated regions with low population density. This means the virus cannot find as many hosts to infect, reducing the potential for spread.
- We’re getting better at rapid local and international responses – better identification of potential outbreaks, better isolation and better strategies to prevent widescale transmission.
But this may not always be the case in the future.
There is always the risk of mutation (especially with RNA viruses) but more importantly, if there is an outbreak in a highly-populated urban area there will be more potential hosts in close proximity to each other and a greater chance of sustained transmission – which could rapidly overwhelm healthcare capacity, making things even worse.
We’ve already had some close calls with Ebola in particular and with Marburg, but remember that population centres such as Mogadishu, Dhaka or even Dubai are a short flight away from areas where VHFs are endemic.
Why do we always ask ourselves ‘is this the new COVID’?
Salience and recency. The pandemic was a massive, disruptive global event that affected every aspect of our lives. Its impact is still fresh in people’s minds and because it had such severe and traumatic consequences, any new outbreak is immediately compared to it.
Pattern recognition and the availability heuristic. Humans are genetically programmed to seek and recognise patterns – even if they’re not there. The availability heuristic is a cognitive bias where people judge the probability of events based on how easily other examples come to mind. Because COVID-19 was so impactful and so recent, it is at the top of our minds when similar events occur.
There are other factors such as coping mechanisms and traditional and social media amplification, but in essence these reactions are driven by a mixture of fear, psychological shortcuts, and an attempt to make sense of new threats in light of a recent, hugely disruptive pandemic.
Vaccines
There are no approved therapies or vaccines against Marburg virus. However there are plans to run trials and treatments organised by members of the Marburg Virus Vaccine Consortium (MARVAC), a group of companies, non-profit organizations and researchers.
Plans for trials were mooted after the 2023 Marburg virus outbreak in Equatorial Guinea which caused 12 deaths among 17 confirmed cases (and another 23 fatal probable cases), but none of the experimental treatments were tested during that outbreak.
Several Marburg virus vaccines are currently in development. The most advanced candidate from the Sabin Vaccine Institute in Washington DC. This uses a modified chimpanzee adenovirus to deliver genetic instructions for human cells to produce a Marburg virus protein, prompting an immune response.
This is the same technology as the AstraZeneca ChAdOx1 COVID vaccine, where an existing virus is genetically reprogrammed to deliver a gene that codes for a Marburg protein that human cells then manufacture to teach the immune system to recognise it.
This is quite literally reprogramming one virus to deliver antivirus software against another virus directly to human cells, that deletes itself like a Snapchat message once the code has been executed.
In an initial trial involving 40 healthy participants in the USA the vaccine was found to be safe, and successfully generated an immune response in most individuals. A larger trial is now underway in Uganda and Kenya to further assess its efficacy.
Another vaccine using similar technology is undergoing initial safety trials in Oxford, and there is another in New York based on an already-approved Ebola vaccine. As yet there are no doses for testing but it is due to go into production imminently.
Given the seriousness of Marburg it is likely that any trial will involve ‘ring vaccination’ – immunising close contacts of an infected individual – rather than a traditional double-blind trial. A ring vaccination strategy was used in the final stages of smallpox eradication.
3,263
Article last updated on Dec 2nd, 2024


