





Monkeypox Virus
Monkeypox virus (MPXV) belongs to the same family as the vaccinia virus, cowpox virus, and variola virus (the causative agent of smallpox).
MPXV is responsible for causing mpox, a disease formerly known as monkeypox. While mpox shares similarities with smallpox, it is significantly less lethal and not as transmissible. The initial symptoms of mpox include fever, headache, body aches, fatigue, and swollen lymph nodes, typically followed by a rash characterised by skin lesions.
This is a rapidly-changing situation and we will endeavour to update this page as new information emerges. Last update: January 30, 2026 13:28
Summary
In 2022, an mpox outbreak occurred in several countries where the virus is not typically found. The infections were mostly mild and primarily affected individuals who had close physical contact with others who were infected.
The 2022 outbreaks were caused by clade II monkeypox virus, the less virulent clade (strain). Also cases in 2022 in non-endemic regions (i.e. outside Central and West Africa) were mainly reported in men who have sex with men (MSM).
That said, it is important to note that anyone in close or intimate contact with an infected person, or who shares towels, bedding etc with them, is at risk of contracting mpox. It’s just that recently it has spread very efficiently in MSM, sex workers and their contacts.
The current outbreak started in the Democratic Republic of Congo (DRC) and involves a more virulent strain (clade I) than the one seen in 2022. Clade I has two subclades, clade Ia and clade Ib.
- In Central Africa, people have been infected with clade Ia mpox through contact with infected dead or live wild animals, household transmission or patient care; a high proportion of cases have been reported in children younger than 15 years of age.
- Subclade Ib was recently identified in eastern DRC and has been spread through intimate and adult sexual contact between different demographics, including heterosexual spread with sex workers. So far, clade Ib seems to have a lower case-fatality rate than clade Ia mpox.
Throughout 2023, reported clade I cases increased significantly in Central Africa, and the number of cases reported so far this year has already outstripped last year’s total.
Confirmed (by laboratory testing) cases will be a significant underestimate of the true numbers due to underascertainment and underreporting.
The current outbreak is more widespread than any previous DRC outbreak, and clade I monkeypox virus has spread to some neighbouring countries where mpox is not considered endemic, including Burundi, Central African Republic, Republic of the Congo, Rwanda, and Uganda. This led to the World Health Organization (WHO) declaring this outbreak a Public Health Emergency of International Concern (PHEIC) on August 14th 2024.
To date, there have been few reported clade I cases outside Africa:
- In October 2025, new unrelated clade I mpox cases were confirmed in Southern California with no history of recent international travel.
- Countries experiencing local human-to-human transmission of clade I mpox include Burundi, Central African Republic, Democratic Republic of the Congo, Kenya, Republic of the Congo, Rwanda, and Uganda.
- Sustained and local person-to-person spread of clade I mpox has taken place in some non-endemic countries through sexual contact, day-to-day household contact, and within the healthcare setting in the absence of personal protective equipment.
- Countries reporting travel-associated cases of clade I mpox include Belgium, Canada, France, Germany, India, Oman, Pakistan, Sweden, Thailand, the United Kingdom, the United States, Zambia, and Zimbabwe.
- Clade II mpox cases continue to spread at low levels in many countries around the world.
Given the prevalence of mpox clade I cases in certain regions of Africa it is entirely unsurprising that cases have arrived elsewhere. It is very likely that more cases will be identified outside Africa over the coming months.
Advice to Productions
MPXV needs very close / intimate contact to be transmitted, so casual contact – e.g. when travelling – is highly unlikely to cause the disease to spread. It definitely doesn’t spread in the same way as SARS-CoV-2.
That said, if you are filming in endemic areas, it is essential to take this risk seriously. But that risk can be minimised by implementing preventive measures, preparing for potential health issues, and ensuring you take current, local advice re prevalence of mpox.
Contrary to some reports, the European Centre for Disease Prevention and Control (ECDC) has not advised vaccination for those travelling to infected areas. Scroll down for more detail.
Confirmed Cases by Country 2024
Numbers are for lab-confirmed cases since Jan 1st 2024 and so will be a significant underestimate.
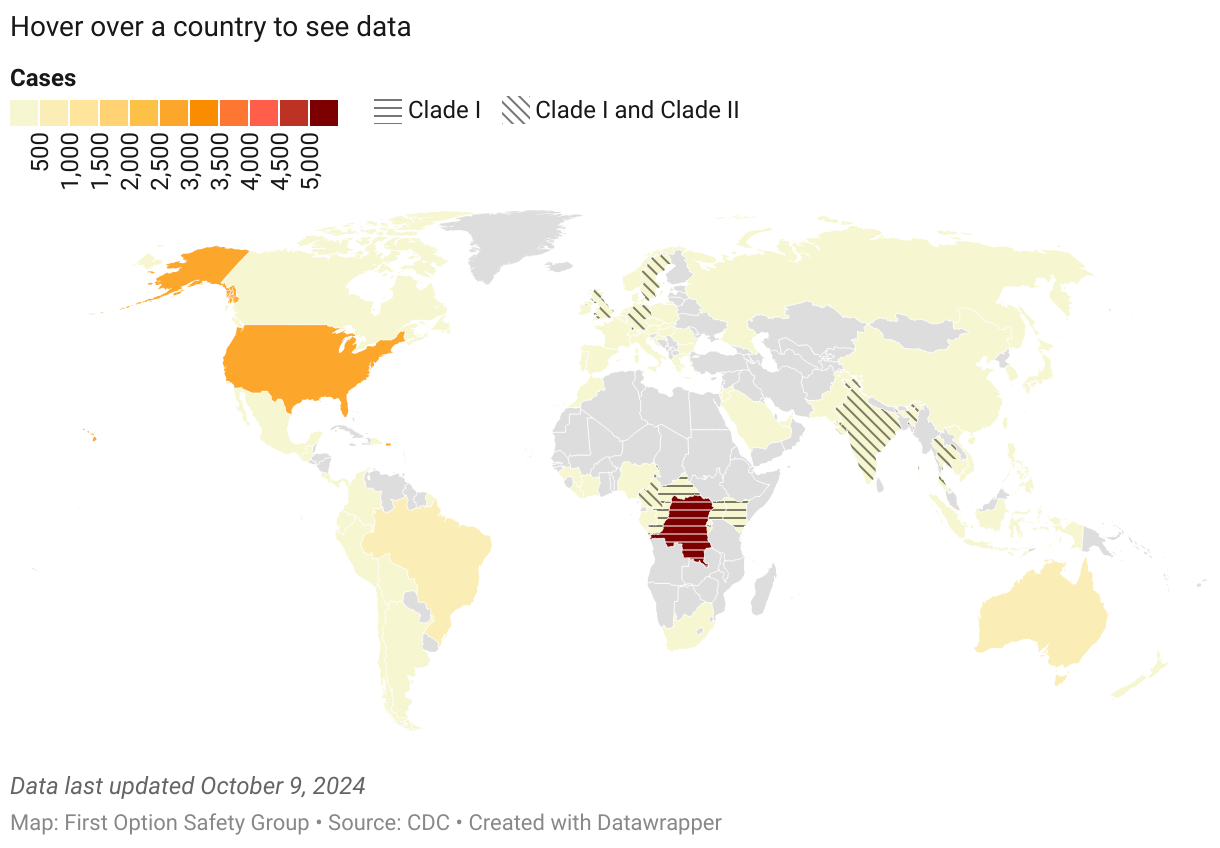
The ongoing global outbreak of clade II mpox has caused more than 100,000 cases in 122 total countries, including 115 countries where mpox was not previously reported. The outbreak was caused by the subclade IIb.
Are YOU at risk?
Answer the questions below to assess your exposure risk in community settings. Each risk level is intended to highlight the need for monitoring and/or seeking clinical advice.
Risk categories last updated August 2nd, 2024.
About MPXV and mpox
Severity
Traditionally, clade II infections carried a 1% case fatality rate (CFR), clade I had a CFR of 10%. It is likely that clade Ib will fall between these figures.
But outside endemic areas, the 2022 outbreak had a CFR under 0.1% due to factors such as better access to healthcare (including effective antiviral drugs and antibody treatments), and not living in countries where immunosuppressive diseases like AIDS and TB are endemic.
Statements that clade 1b is ‘more virulent’ are premature, unhelpful and are only speculation until we see how it behaves in people. Additionally, outcomes for individuals with access to proper healthcare provision can be very different to those in endemic areas.
But mpox disease can still be very painful and potentially disfiguring. In 2022, outside Africa a minority of cases (~10%) were hospitalised for isolation, pain management, or for complications such as secondary skin infections, abscesses, and difficulty in swallowing. Less severe but more common complications included rectal pain, swelling of the penis, and secondary bacterial infections.
Incubation and Spread
A person can spread mpox from the time symptoms start until the rash has fully healed and a fresh layer of skin has formed. There is no evidence to suggests people who never have symptoms can spread the virus to someone else.
The principal mode of transmission is intimate contact principally via sexual networks, but additionally via close contact. This includes spread within households (often to children) or when nursing someone with the disease without using adequate PPE. This could conceivably include prolonged face-to-face interactions with someone with active disease – but in general MPXV is not spread via the respiratory route.
- The monkeypox virus can also spread through contact with objects, fabrics, and surfaces that haven’t been disinfected after being used by someone with mpox. This includes items such as clothing, bedding, towels, fetish gear or sex toys.
- MPXV can also spread from animals to people via small wild animals in West and Central Africa where mpox is endemic. Transmission can occur on direct contact with an infected animal, fluids or waste, or getting bitten or scratched, or during activities like hunting, trapping, or processing infected wild animals in areas where mpox is endemic.
- It can also spread during pregnancy via the placenta.
Two healthcare workers developed lesions on their hands after visiting a patient at home. They only donned gloves when they were ready to take samples and had been touching multiple surfaces until then. Despite being in close contact with the patient, the spread was due to touching surfaces contaminated with virus particles (‘fomite transmission’) and not respiratory transmission.
No link has been established between mpox and pools, hot tubs and spas. Provided chorine is within recommended levels it will render the virus inactive.
Symptoms
Individuals with mpox commonly develop a rash that can appear on the hands, feet, chest, face, or mouth, as well as near the genitals, including the penis, testicles, labia, vagina, and anus.
The incubation period for the virus is 3 to 17 days, during which a person may not experience any symptoms and may feel completely well. There are unconfirmed case reports that symptom onset can be as little as 2-4 days with this clade.
The rash progresses through several stages, eventually forming scabs before healing. At first, the rash may resemble pimples or blisters that can be painful or itchy.
Other symptoms:
- Swollen lymph nodes
- Fever
- Chills
- Tiredness
- Muscle aches and backache
- Headache
- Respiratory symptoms such as a sore throat, congestion, or cough.
Stages
There are 3 stages: incubation period, prodrome, and rash.
- Incubation: infection with monkeypox virus begins with an incubation period where the person does not have symptoms and may feel fine. The incubation period is usually 1-2 weeks but it may be shorter with clade Ib. A person is not contagious during this period.
- Prodrome: people with mpox may develop an early set of symptoms (prodrome). Symptoms may include fever, malaise, headache, sore throat, or cough, and (in many cases) swollen lymph nodes (lymphadenopathy is a characteristic feature of mpox and differentiates it from smallpox), lymph nodes may swell in the neck, armpits (axillary), or groin (inguinal) and can occur on both sides of the body or just one. A person may be contagious during this period and should isolate if they develop symptoms.
- Rash: in some recent cases, people have presented with a rash without a recognised prodrome. Many of the recent cases have only had localised lesions and have not presented with a more diffuse rash. People with mpox infection develop lesions that typically progress from papules (flat lesions), macules (raised, firm, painful lesions), vesicles (filled with clear liquid), pustules (filled with pus), and then scabs. A person is contagious until after all the scabs on the skin have fallen off and a fresh layer of intact skin has formed underneath.
The virus is found in the lesions which is why contagiousness correlates with the rash. Note that lesions can be present in the mouth and nose, hence the risk of transmission via spit and snot.
It’s also conceivable that there may be virus on the skin before the rash is easily visible, hence the advice to isolate during the prodrome phase in (2) above.
Testing
There are PCR tests but these tend to be limited to confirming a clinical diagnosis, not for screening. This is principally because the medic needs to sample an actual lesion for testing.
Close Contacts
If you are a close contact of a person with mpox, it’s important to take the following steps:
- Watch for symptoms of mpox for 21 days after your last exposure. The rash can initially look like pimples or blisters and is often painful or itchy. Sometimes people have flu-like symptoms before the rash. Some people get a rash first, followed by other symptoms. Some people only experience a rash.
- Get vaccinated, if available. In the UK, the NHS mpox outbreak vaccination programme ended in July 2023, but it is still available in London and Greater Manchester to eligible people who live in London or Greater Manchester or regularly travel to London or Greater Manchester to have sex. It is likely that post-exposure prophylaxis may be made available and the groups most at risk generally have good links with sexual health provision.
You can also use our risk checker above.
Avoiding Infection with MPXV
All types / clades of MPXV can spread through direct contact with infected wild animals, through close contact (including intimate or sexual contact) with a person with mpox, and through contact with contaminated materials.
A recent report from the US Centers for Disease Control and Prevention (CDC) indicated that 67% of suspected DRC mpox cases and 78% of suspected mpox deaths occur in people aged 15 years and younger, but the recent uptick includes person-to-person transmission, principally in men who have sex with men (MSM), sex workers and their contacts.
Transmission of MPXV can be dramatically reduced by:
- Refraining from close contact with individuals who exhibit signs and symptoms of mpox, especially those with skin or genital lesions.
- Steering clear of wild animals – alive or dead – in regions where mpox is common.
- Avoiding contact with items contaminated by sick individuals, such as clothing, bedding, or materials from healthcare settings, or that have come into contact with wild animals.
- Refraining from consuming or preparing meat from wild animals (bushmeat).
Mpox occurs mostly in central and western Africa, but if you have a new or unexplained rash or other mpox symptoms and you have been involved in one of the high risk activities above, you should seek medical advice.
Clades
MPXV virus variants are referred to as clades: clade I (formerly known as the Congo Basin or Central African clade) and clade II (formerly known as the West African clade). Clade II is further divided into subclades: clade IIa and clade IIb.
The virus was first described in 1958 in two outbreaks of a pox-like disease among colonies of research monkeys. The first human case of mpox was recorded in 1970 in the DRC. The disease is endemic in central and western Africa.
According to the WHO, cases identified as part of the ongoing (since 2022) global outbreak are largely caused by clade IIb. Clade I is responsible for infections in the DRC and is estimated to cause more severe disease and higher mortality than clades IIa and IIb.
Clade I causes the same disease as clade IIb (the variant behind the outbreak that escaped Africa in 2022) but it is often associated with a higher risk of a more severe course of disease and higher mortality.
The previous global outbreak of clade IIb has mainly been spread through sexual contact, while clade I is more commonly spread through other contact routes, mainly close contacts within the household and often to children, however it seems that the current cases of Clade 1 infection are likely due to sexual transmission.
Q&A: Clade 1b
The clade 1b outbreak is believed to have originated in Kamituga, a mining town in South Kivu province. A 2024 study found that most of the initial surge of cases occurred among sex workers. (Children with clade I mpox tend to be infected with Ia, likely via household contact).
Little is known about the natural history and transmission dynamics of the new clade Ib variant, and while this information is important to inform the control strategies, commentary around clade Ib’s virulence compared with other strains in the clade is speculation at this stage.
To understand factors such as mortality rate we need to understand better the number who are infected overall, including those with milder disease and the relationship between transmission route and severity of disease. Also, this disease impacts highly vulnerable communities and there is already much stigma associated with this.
The situation is concerning because of the spread of the clade 1b virus, which is considered to cause more severe disease, and because there are many children being infected in DRC during this new outbreak. 40% of cases are in children under 5 years old.
As mpox disease is more severe in immunocompromised individuals, it is also a concern that the current outbreak is taking place in a region where HIV prevalence is relatively high but access to antiretroviral drugs is poor.
Is there a Vaccine?
There are three, plus some antiviral medications. One of these is TPOXX (Tecovirimat) but has not improved clade Ib symptomatic relief in the DRC but may reduce mortality.
The smallpox vaccine Jynneos™ (MVA-BN) has reasonable efficacy against MPXV. It is made using weakened live vaccinia virus and cannot cause smallpox, monkeypox, or any other infectious disease. It requires two doses, four weeks apart.
Another smallpox vaccine, LC16m8 – licenced in Japan – is a single-dose replicating attenuated strain of vaccinia. There is an older, second generation vaccine called ACAM2000 too.

Supplies are very limited; this represents a major bottleneck for control strategies. The amount of vaccine required has been estimated by Africa CDC to be 10 million doses.
There is a new RNA lipid nanoparticle vaccine in trial, mRNA-1769. Tests in animal models resulted in fewer lesions and reduced viral replication, and induced enhanced neutralizing and functional antibodies compared with MVA. This is promising, but it will be some time before we see it in peoples’ arms. And it will be even longer before we know how long protection may last.
Even were there sufficient doses of any vaccine, there are issues of cost and difficulties deploying a vaccination programme in high-conflict areas, but the additional tragedy here is that this is yet another emerging infectious disease where the response from the WHO and the West is tepid until it leaves Africa.
Is This ‘The New COVID’?
No. The data thus far suggests that Ib is being transmitted principally via sexual intercourse rather than intimate or household contact. The 2022 outbreak also spread via sexual networks where people have multiple sexual partners, which helped it spread efficiently and rapidly.
Unlike SARS-CoV-2, MPXV is not airborne. So the COVID era risks associated with traveling, public transport, and congregating in public spaces or offices quite simply aren’t there.
Also the 2022 mpox outbreak slowed predominantly due to changes in behaviour by at-risk populations rather than vaccines. It’s worth noting that a key difference between the transmission of smallpox and monkeypox viruses is that there was airborne transmission of smallpox virus. This isn’t a feature of monkeypox virus and viruses don’t mutate to develop a new mode of transmission. It doesn’t work that way.
Now that we’ve seen a case in Europe it’s a near-certainty we’ll see a drip – drip of cases. But because of the way MPXV is transmitted, if anyone is anticipating a wave or a tsunami of infections they will be disappointed.
Has the ECDC Called for Vaccination for Travellers?
No. It has advised public health authorities to offer vaccination to “eligible unvaccinated high-risk individuals for sexual transmission” should there be a wider outbreak in the EU, and its advice to travellers visiting affected areas is:
- Consult guidance from your national health authorities, ECDC guidance and epidemiological information;
- Avoid contact with wild animals;
- Refrain from sexual or other close contact with individuals with possible or known mpox infection and those with visible lesions or other mpox-compatible symptoms;
- Consult national guidelines on vaccination against mpox before travel.
You can read the full ECDC Risk Assessment below.
I’ve had chickenpox. Am I immune?
No. Chickenpox is caused by Varicella zoster virus (VZV), a type of herpesvirus. Although both are part of a broader family of poxviruses, they are very distinct in their structure so there is no cross-immunity. However the variola virus (which was used to vaccinate against smallpox) is sufficiently similar to give immunity against MPXV.
Another pox – historically known as the ‘Great Pox’ – won’t give cross-immunity either: it’s not even caused by a virus, it’s caused by a spirochete, Treponema pallidum. The disease had a number of names over the centuries: most Europeans called it the ‘French Disease’, except the French who called it the ‘Italian Disease’ but now everyone seems to have settled on ‘syphilis’.
Monkeypox Virus | International Advice
5,551
Article last updated on Jan 30th, 2026


